Unit A - Part 1 : Malocclusion: what is it and why should we treat it?
Describe ideal occlusion regarding tooth relationship to the line of occlusion.
Angle’s Description of “line of occlusion” Lecture, Contemporary Orthodontics (sixth edition) TOC
- Angle used specific suffixes to identify tooth positions:
- Bucco-version
- Linguo-version
- Labio-version
- Torsio-version (rotation)
- “The line of occlusion is a smooth (catenary) curve passing through the central fossa of each upper molar and across the cingulum of the upper canine and incisor teeth. The same line runs along the buccal cusps and incisal edges of the lower teeth, thus specifying the occlusal as well as interarch relationships once the molar position is established” (“Contemporary Orthodontics (sixth edition)”, p. 13) (pdf)
/image-44PT89UH.png)
- “Note that the Angle classification has four classes: normal occlusion, Class I malocclusion, Class II malocclusion, and Class III malocclusion. Normal occlusion and Class I malocclusion share the same molar relationship but differ in the arrangement of the teeth relative to the line of occlusion. The line of occlusion may or may not be correct in Class II and Class III malocclusion.” (“Contemporary Orthodontics (sixth edition)”, p. 12) (pdf)
Describe ideal occlusion in transverse, antero-posterior, and vertical planes.
Ideal Occlusion in the A-P Plane
/image-XN8D5MLB.png)
- Posterior Occlusion in the anterio-posterior plan is defined by the molar relationship.
- Divided into 4 classes (Angle’s):
- Class I (normal occlusion): Mesiobuccal cusp of maxillary fist molar occludes in the buccal groove of the lower first molar
- Class I Malocclusion: Molar relationships remain the same but differ in the arrangement of teeth relative to the line of occlusion.
- Class II Malocclusion: Lower molar distally positioned relative to upper molar, line of occlusion not specified
- Class II Division 1: Proclined maxillary incisors (increased overjet); associated with convex profile and lip incompetence
- Class II Division 2: Retroclined maxillary incisors + proclined lateral incisors; associated with a deep bite
- Class III: Lower molar mesially positioned relative to upper molar, line of occlusion not specified
- Divided into 4 classes (Angle’s):
- Anterior occlusion in the anterio-posterior plane is defined by overjet
- Overjet: the horizontal overlap of the incisors
- Normally the incisors are in contact, with the upper incisors ahead of the lower by only the thickness of their incisal edges (i.e., overjet of 2 to 3 mm is the normal relationship).
- If the lower incisors are in front of the upper incisors, the condition is called reverse overjet or anterior crossbite.” (“Contemporary Orthodontics (sixth edition)”, p. 16) (pdf)

- Overjet: the horizontal overlap of the incisors
Ideal Occlusion in the Transverse Plane
- Occlusion in the transverse plane is dictated by the location of the posterior teeth.
- Normal transverse occlusion is: Upper teeth buccal to lower teeth (i.e. BULL Rule )
- The most common major deviation from the transverse dental relationship is lingual posterior crossbite
- Lingual posterior cross bite: upper teeth lingual to the lower teeth
Ideal Occlusion in the Vertical Plane
- Ideal Occlusion in the vertical plane is measure by overbite
- Overbite is defined as the vertical overlap of the incisors
- Normally the lower incisal edges contact the lingual surface of the upper incisors at or above the cingulum
- there is normally a 1 - 2 mm overbite
- In open bite, there is no vertical overlap and the vertical separation of the incisors is measured to quantify its severity
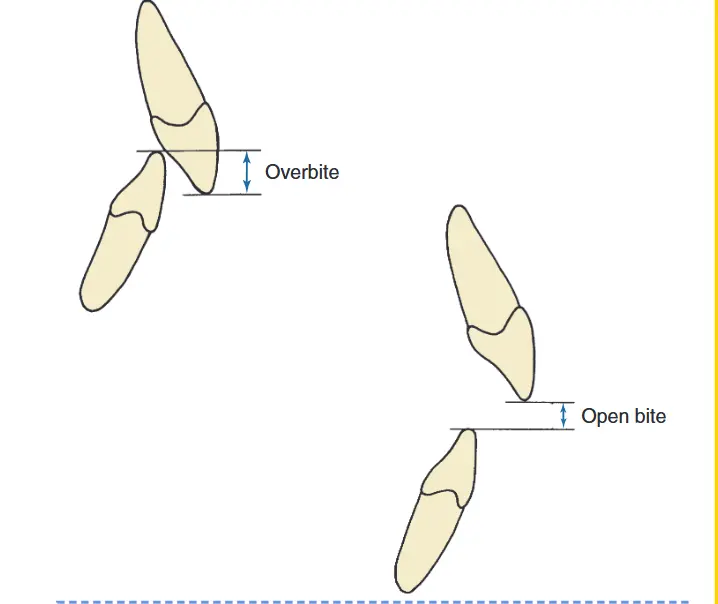
- Normally the lower incisal edges contact the lingual surface of the upper incisors at or above the cingulum
List dental characteristics for the Angle classification and discuss its advantages.
See above
Describe functional, health, and psychosocial reasons for treatment.
Primary Objectives for Orthodontics
- Reduce psychosocial handicap
- Improve oral function
- Adjunct to disease control (not to treat disease )
Describe realistic goals for orthodontic treatment and their evolution.
The modern objectives for orthodontic treatments fall under the “Soft Tissue Paradigm”
- Treatment goals of the soft tissue Paradigm
- Normal soft tissue proportions and adaptations
- Functional occlusion is a secondary goal
Historically the angle paradigm for ideal dental occlusion was to have an ideal dental occlusion and skeletal relationships. This goal has shifted to the soft tissue paradigm in the modern era because a patients appearance is often much more of concern to them and functional occlusion can still occur even if the scheme is not ideal.
| Feature | Angle Paradigm | Soft Tissue Paradigm |
|---|---|---|
| Primary goal of treatment | Ideal dental occlusion | Ideal soft tissue proportions and adaptation |
| Secondary goal of treatment | Jaw relationships | Functional occlusion |
| Hard vs soft tissue relationship | Ideal skeletal/dental produces ideal soft tissue | Ideal soft tissue defines ideal skeletal/dental |
| Diagnostic emphasis | Dental casts, cephalometric x-rays | Clinical examination of soft tissues |
| Treatment approach | Obtain ideal dental and skeletal relationships, and the soft tissues will be OK | Determine ideal soft tissue relationships, and then place the jaws and teeth as needed to obtain them |
Modern Patient Perception
Patients often identify themselves by their profile in the mirror rather than molar relationships. Modern standards favor fuller profiles (e.g., the "Angelina Jolie era") over the straight or concave profiles favored in the past.
Discuss treatment need versus demand in the current environment.
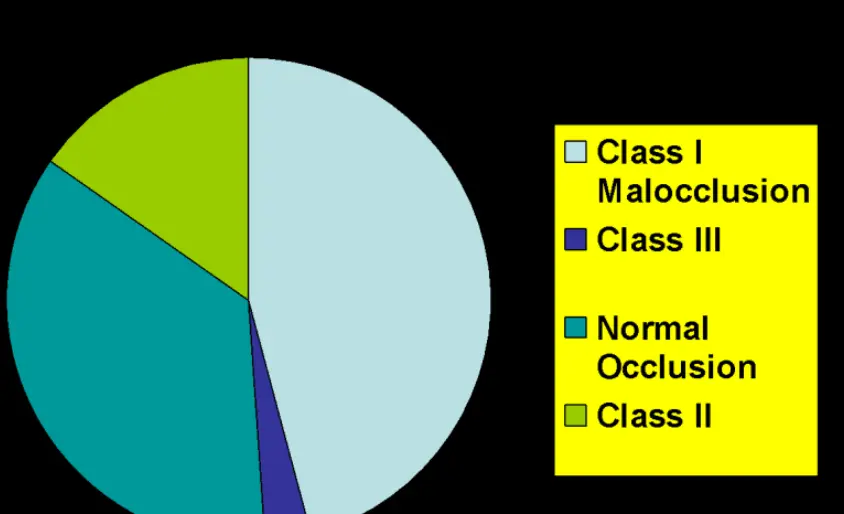
Treatment Need 01 - Malocclusion Definition and Prevalence The key points to remember from modern population studies of malocclusion:
-
About half the population have well-aligned teeth or slight irregularity, while about 15% have irregularity severe enough that either major expansion of the dental arches or extraction of a permanent tooth in each quadrant of the arch is likely to be needed if the teeth are to be aligned.
-
With increasing age, incisor irregularity gets worse and the number of people with ideal alignment decreases.
-
15% of the US population are Class II, and about half of these individuals have overjet severe enough to predispose them to problems in social interactions.
-
Open bite is much more prevalent and deep bite less prevalent in African-Americans.
-
Class III and reverse overjet are much more prevalent in those of Asian descent.
-
Other racial / ethnic differences are modest and unimportant.
Who seeks Orthodontic treatment
- 65% of the population have malocclusion
- Dentists feel that 55% need treatment
- Patients feel that 35% need treatment
 **Treatment Acceptance Rates **
**Treatment Acceptance Rates **- 55% need treatment
- 50% accept treatment at no cost
- 5% wouldn’t accept treatment even if it was free
Increasing Treatment Demand
Older patients are more likely to want orthodontic treatment now. Some say its because its more socially acceptable although no one can say why