Dental Trauma: Primary Dentition
Course Information1
- Module: DENT 5312 Paediatric Dentistry Module
Lecture Focus
This lecture focuses on the management of traumatic dental injuries in the primary dentition, emphasizing the high frequency of these cases in general practice and the necessity of a systematic approach to diagnosis, documentation, and treatment to protect the developing permanent dentition.
Questions to ask when a dental trauma case presents itself
- Prevalence : How common is this?
- Examination: What should I look for?
- Manifestations: What are the different types of trauma
- Treatment: What should I do?
- Sequelae : What should I tell the parent?
Prevalence of Injuries
Statistical Overview2
-
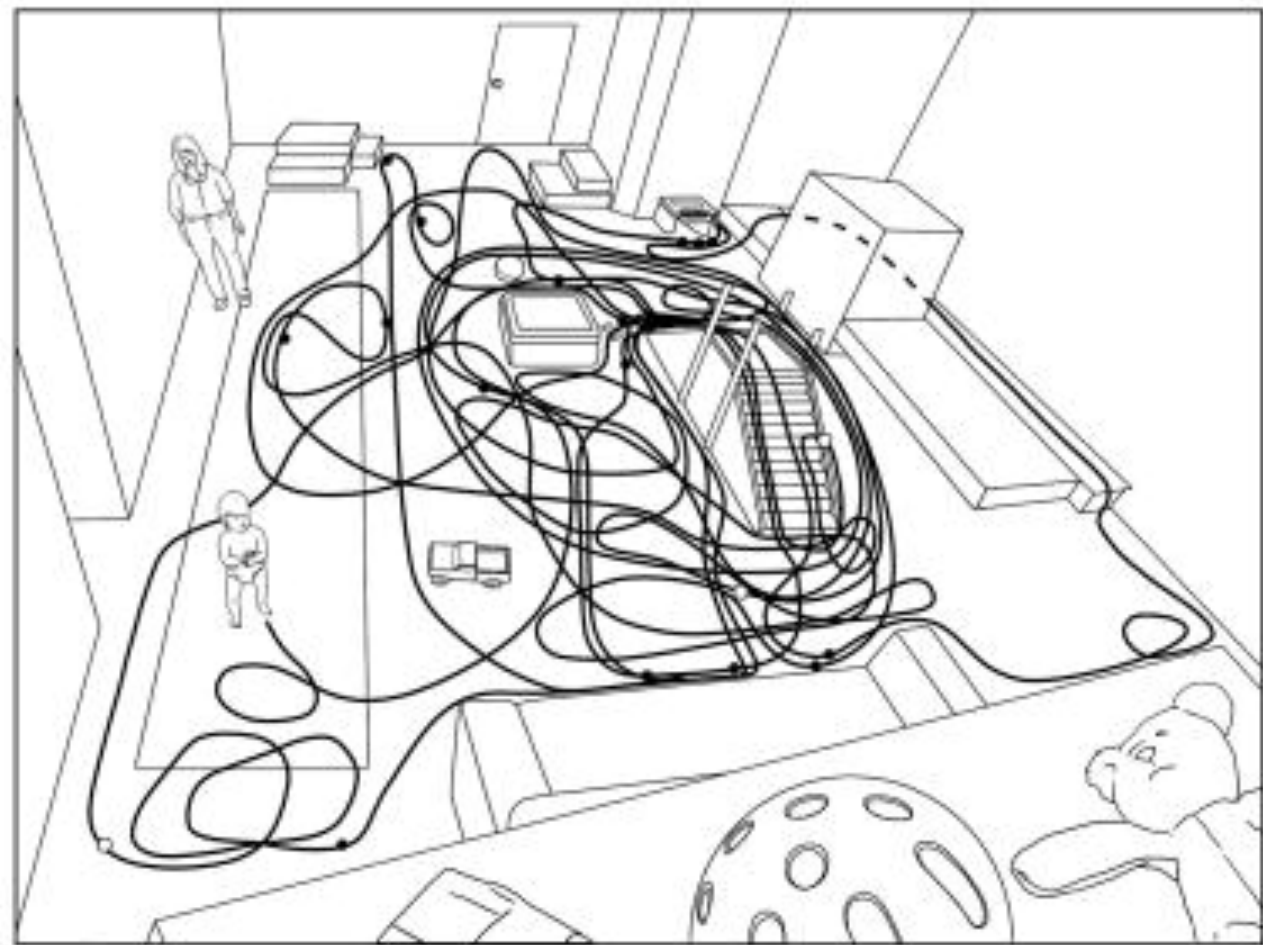
In preschool children, head and facial injuries account for 40% of all somatic injuries (Glendor et al. 1996).
-
Toddlers fall an average of 17 times per hour (Adolph et al. 2012).
-
While toddlers fall due to instability, older children experience higher-velocity impacts from activities involving bicycles, scooters, and playground equipment (e.g., monkey bars).
 |  |
Injury Frequency3
-
30% of children sustained injuries specifically to primary teeth.
-
46% of children had a history of traumatic injuries involving primary and/or permanent teeth (Andreasen and Ravn 1972).
-
In the primary dentition, luxation injuries (displacements) are significantly more common than fractures.
-
According to Heinz, concussion, subluxation, and luxation account for about 80% of primary tooth injuries. This is due to the softer, more pliable alveolar bone in young children, which allows teeth to displace rather than fracture.
Clinical Examination
A rational examination procedure is essential to establish a complete and correct diagnosis of all soft and hard tissue injuries.
Initial Preparation and History4
-
==Calm the Environment: Trauma cases are often distressing for both the parent and the child. Practitioners should take deep breaths and maintain a calm demeanor.==
-
Clean the face and oral cavity: Use water or saline. For soft tissue wounds, use a mild detergent to improve patient comfort and facilitate the examination.
-
Use warm water and gauze to clean the child's face and oral cavity. Because the gingiva is highly vascular, even minor trauma can produce significant bleeding, making the injury appear worse than it is.
-
Medical and Dental History: Identify allergies, blood disorders, or previous dental traumas that may explain radiographic findings like pulp canal obliteration or apical pathology.
-
Use a standardized template to ensure no critical details are missed, including comprehensive allergy and trauma history.
Diagnostic Questions
- Where did the injury occur? Relevant for legal implications and identifying potential contamination
- ==Why did the injury occur? Understanding the context helps complete the clinical picture and distinguish between accidental and non-accidental injuries.==
- How did the injury occur? Helps identify impact zones (e.g., a chin injury often correlates with premolar/molar fractures
- During the extraoral examination, specifically check for chin point trauma, as this often correlates with molar or condyle fractures.).
- When did the injury occur? Critical for treatment decisions, especially regarding extraoral storage time for avulsed teeth.
- Was there unconsciousness? Amnesia, nausea, and vomiting are signs of brain damage requiring medical attention
- Ask specifically about loss of consciousness, vomiting, or nausea, as these symptoms indicate a potential head injury requiring immediate referral to an Emergency Department.
- Is there a bite disturbance? May indicate luxation, displacement, alveolar/jaw fractures, or condylar fractures
- A "step defect" in the bite may indicate an alveolar or jaw fracture.
- Is there sensitivity to temperature? Positive findings indicate exposed dentin or pulp.
Clinical Assessment Steps
- Soft Tissue: Examine face, lips, and oral muscles for lesions.
- Look specifically for "degloving" injuries or embedded tooth fragments in the lips or cheeks.
- Skeletal: Palpate the facial skeleton for fractures.
- Dental Region: Inspect for fractures, abnormal positioning, mobility, and percussion response. Note displacement direction and relationship of fractures to the gingival sulcus or pulp.
- ==Intraoral: Check the floor of the mouth for hemorrhage (potential symphyseal fracture) and observe the range of motion and deviation during mouth opening.==
- Pulp Testing: Complete the examination with electrometric pulp testing.
Radiographic Examination
Multiple radiographic procedures are necessary to detect tooth displacement in the socket and the presence of root fractures.
Limitations of 2D Imaging
Standard periapical views are two-dimensional and can easily miss fractures due to angulation challenges.
Radiographic Techniques and Film Formats5
- Steep Occlusal Exposure: Using a size 2 film (DF 58, EP 21). Provides an excellent view of lateral luxations, apical and mid-root fractures, and alveolar fractures.
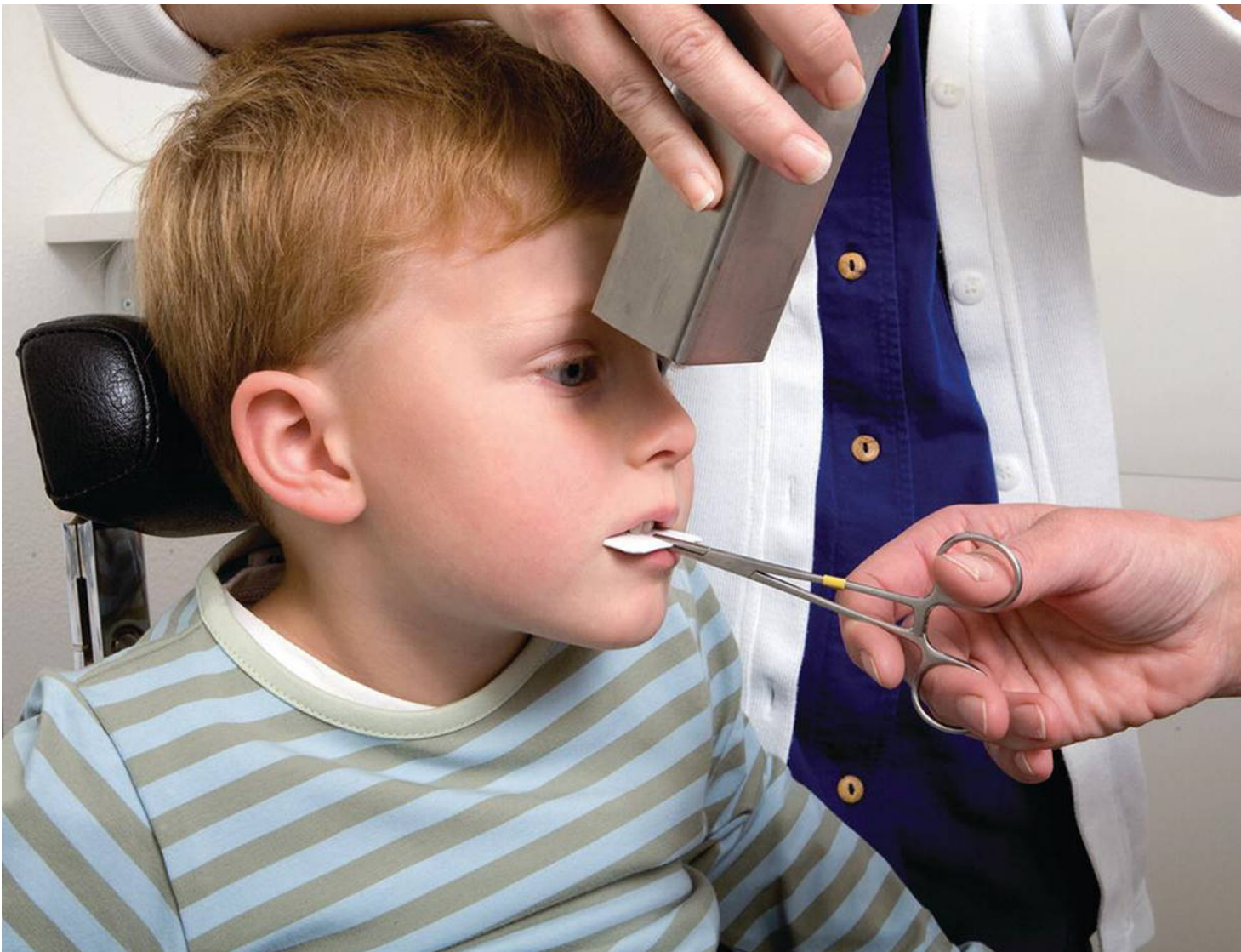
- While size 4 (occlusal) film is ideal, a size 2 film can be positioned horizontally for toddlers to achieve adequate imaging.
- Periapical Bisecting Angle Exposure: Using a size 1 film (DF 56, EP 11) for each traumatized tooth. Provides information on cervical root fractures and other displacements.
Recommended Examination Protocol
A comprehensive examination of the incisor region should comprise (this is called a trauma series):
- One steep occlusal exposure.
- Three periapical bisecting angle exposures.
Clinical studies emphasize that multiple radiographic views are required to accurately identify displacement and root fractures.
Managing Pediatric Anxiety
Use a teddy bear to demonstrate the X-ray machine to the child (Tell-Show-Do technique) to reduce anxiety and improve cooperation.
Standard Imaging Views6
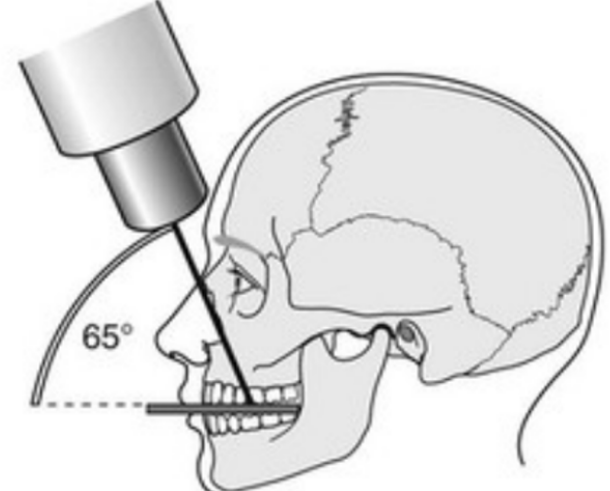
- Steep Occlusal Exposure (Size 2 film): Best for detecting lateral luxations, apical/mid-root fractures, and alveolar fractures.
- ==This view is taken at a 65-degree angulation and is the most effective for detecting the majority of primary tooth fractures and displacements.==
- Periapical Bisecting Angle Exposure (Size 1 film): Essential for identifying cervical root fractures and specific tooth displacements.
- ==Lateral View: Occasionally used to determine if an intruded root has been forced through the buccal plate.==
 |  |
 |
Summary of Protocol
To provide sufficient diagnostic information for the incisor region, the examination should include one steep occlusal exposure and three periapical bisecting angle exposures.
- ==Position the film horizontally and have the child bite gently, supported by the parent or using tongue depressors to protect digital sensors. This protocol helps identify incidental findings, such as a mesiodens (supernumerary tooth), and clarifies the relationship between the primary root and the permanent follicle.==
Photographic Examination and Screening
Screening for Non-Accidental Injury7
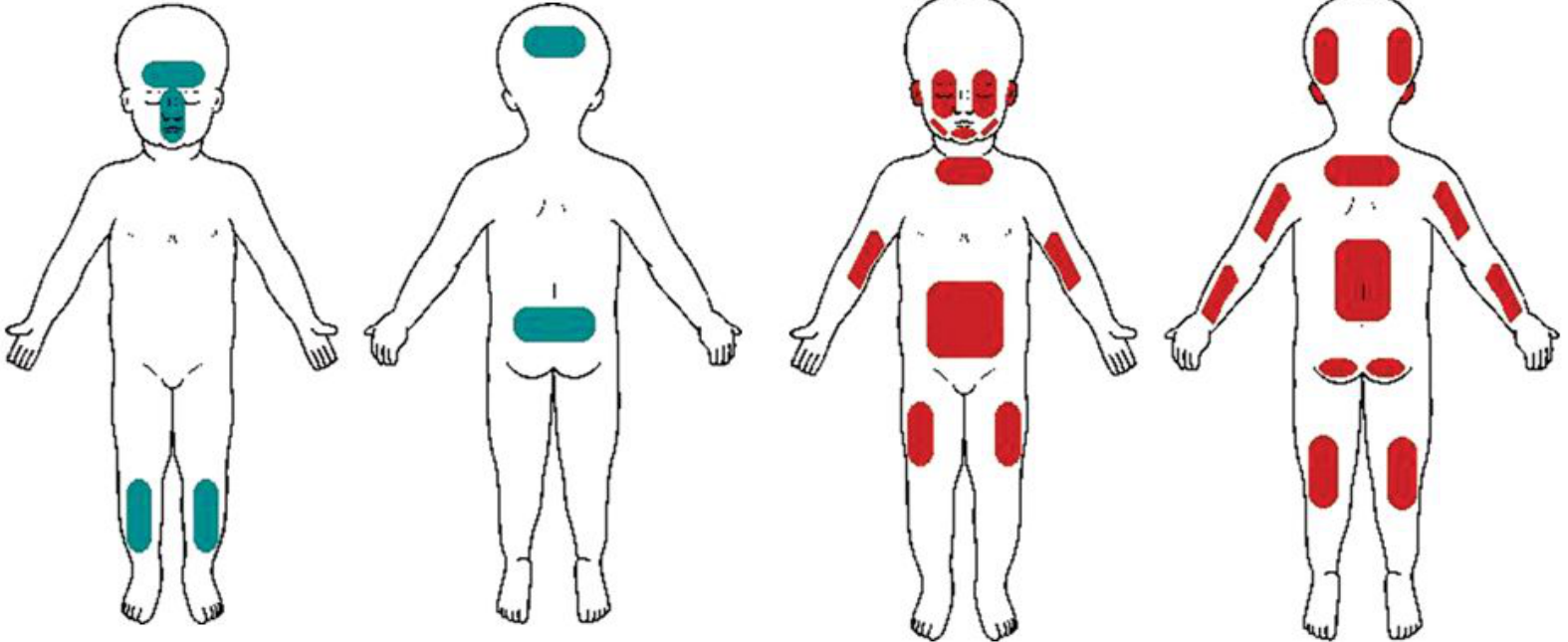
When performing a photographic examination, it is critical to distinguish between accidental and suspicious bruising patterns:
-
Meticulous photographic records are essential for long-term monitoring and legal protection.
-
Accidental Bruising: Typically located in peripheral areas.
-
Non-Accidental Bruising: Typically located in central areas of the body (Santos et al. 2007
Red Flags for Non-Accidental Injury
Bruising patterns on the face, arms, or neck that are inconsistent with the provided history or the mechanism of the dental injury may indicate child abuse. Practitioners must act on these red flags.).
 |  |
Classification of Injuries
Fractures
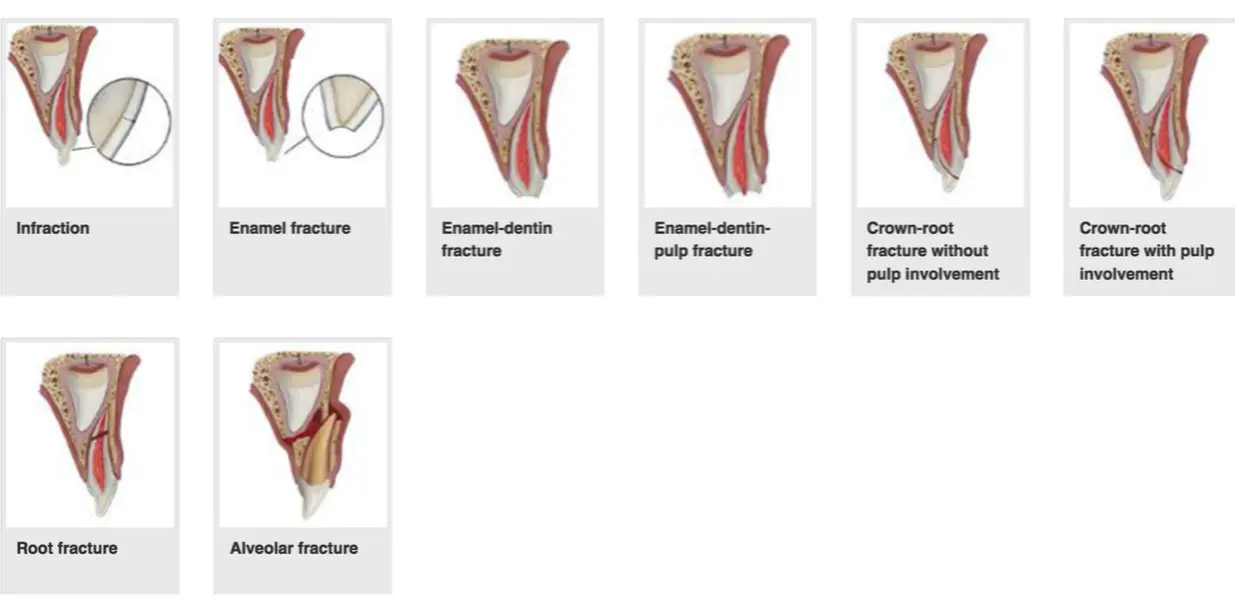
Classification of Fractures8
- Infraction
- Enamel fracture
- Enamel-dentin fracture
- Enamel-dentin-pulp fracture
- Crown-root fracture (with or without pulp involvement)
- Root fracture
- Alveolar fracture
Alternative Classification with Definitions
- Enamel Infraction: Incomplete fracture (crack) without loss of structure.
- Uncomplicated Crown Fracture: Involves enamel or enamel/dentine without pulpal exposure.
- Complicated Crown Fracture: Involves the pulp.
- Root Fracture: Horizontal or vertical fractures of the root.
- Alveolar Fracture: Fracture of the bone socket.
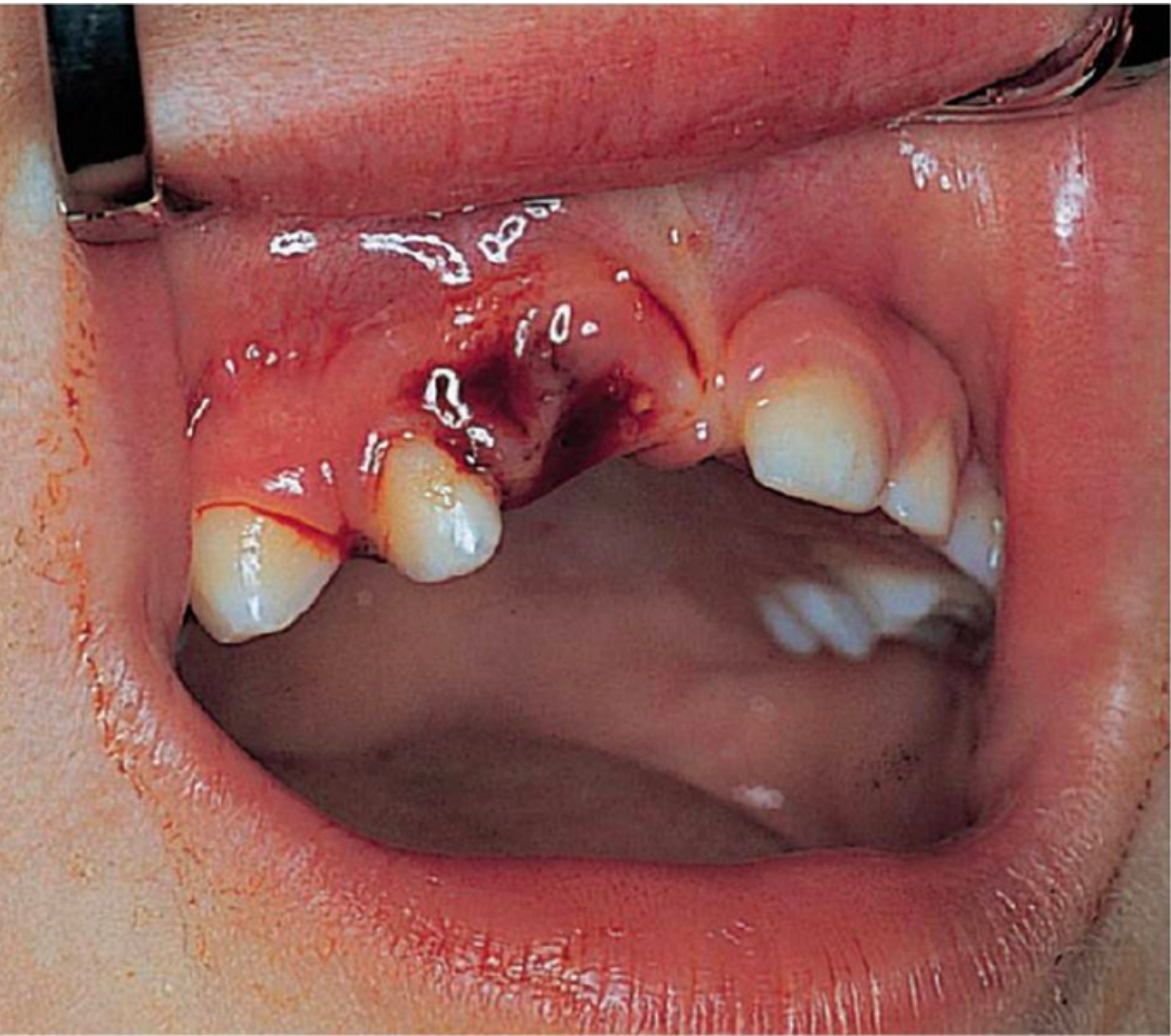
Luxations
- Concussion and subluxation is hte most common type of primary traumatic injury
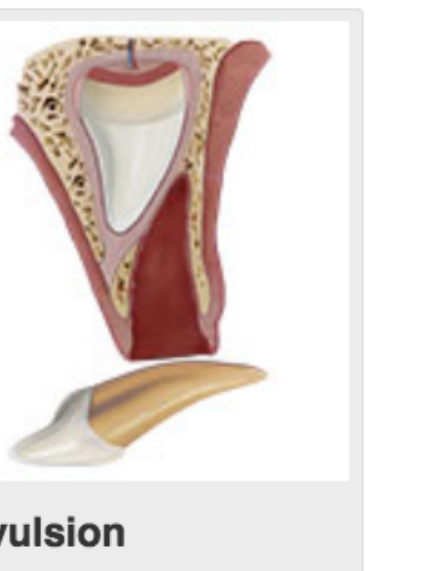
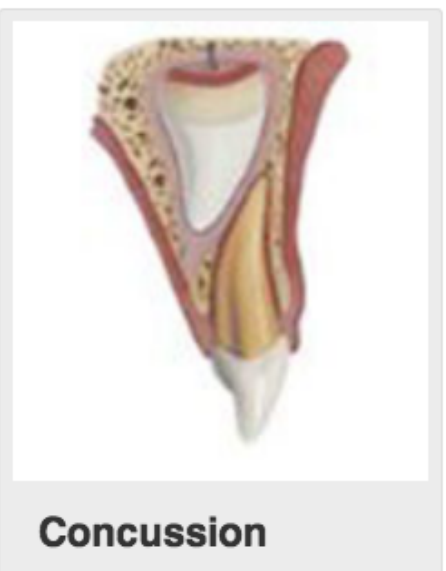
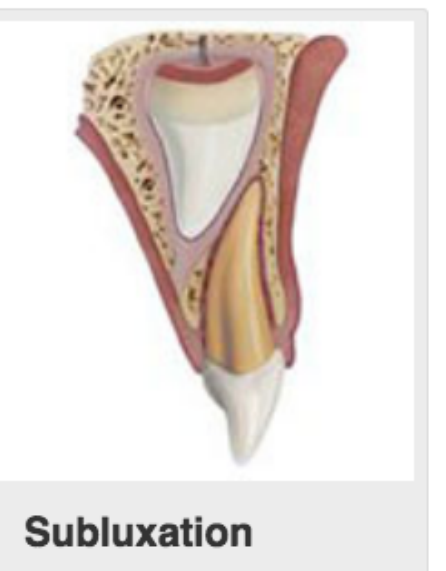
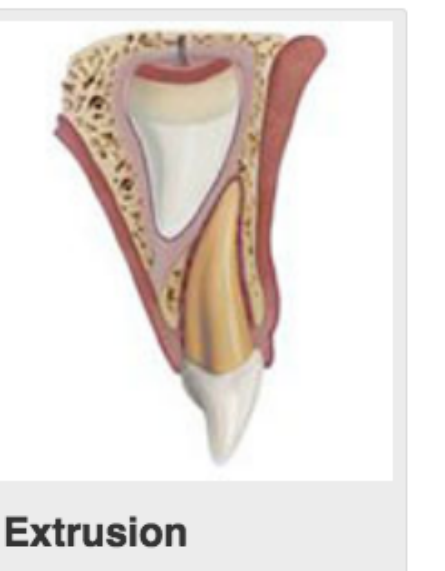
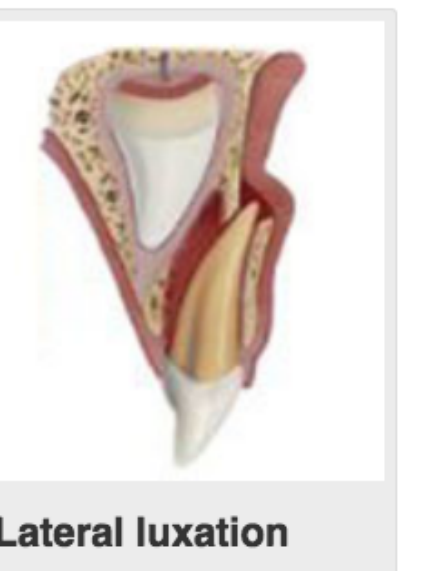
Classification of Luxation Injuries9
- Concussion: Injury to the tooth-supporting structures without increased mobility or displacement. Tender to touch.
- Subluxation: Injury resulting in increased mobility but without displacement. Bleeding at the gingival crevice is common.
- Extrusion: Partial displacement of the tooth out of its socket (apical displacement).
- Lateral Luxation: Displacement of the tooth in a direction other than axially (horizontal displacement). Often accompanied by a fracture of the alveolar bone.
- Intrusion: Displacement of the tooth deeper into the alveolar bone (coronal displacement of the root).
- Avulsion: Complete displacement of the tooth out of its socket.

 |  |  |
 |  |  |
Treatment Options10
Treatment for primary dentition trauma generally follows two paths (Andersson et al. 2012):
-
Conservative Management
- Soft diet and analgesia.
- Ongoing review and monitoring.
-
Extraction
- Indicated based on the extent of injury.
- Necessary for occlusal interference or pulpal exposure.
- Required for degloving injuries.
Conservative Management
Concussion and Subluxation11
- Management: Soft diet, analgesia, and ongoing monitoring.
- Hygiene is also an essential component of the management protocol. So you can give chlorhexidine gel, so if the yreally can’t get the brush in on the first day they can use hteir finger and every other day after use a brush (chlorhexidine for the firs tweek only)
- Risk Profile: Low risk of complications (less than 10%).
- Potential Complications: Pulp necrosis, resorption, pulp canal obliteration (PCO), and premature loss.
- Timeline: Most complications occur within the first 12 months.
- Recall schedule: 1 week, 1 month, 3 months, 6 months, 1 year
- Demographics: Complications are more likely in children over 4 years of age (Lauridsen et al. 2017).
- This is due to physiological root resorption and easier bacterial ingress.
 |  |
 |
Intrusion Management12
- Spontaneous Re-eruption: Occurs in 80% of intruded primary teeth.
- This occurs even if 100% intruded.
- Complication Rate: Approximately 1/3 will develop complications such as infection or ankylosis.
- Risk Factors (Lauridsen et al. 2017):
- Lowest risk of pulp necrosis in children under 2 years of age.
- The degree of intrusion or presence of a concomitant fracture does not significantly affect the complication rate.
- Monitoring is essential at 1 week, 1 month, 3, 6, 9, and 12 months.

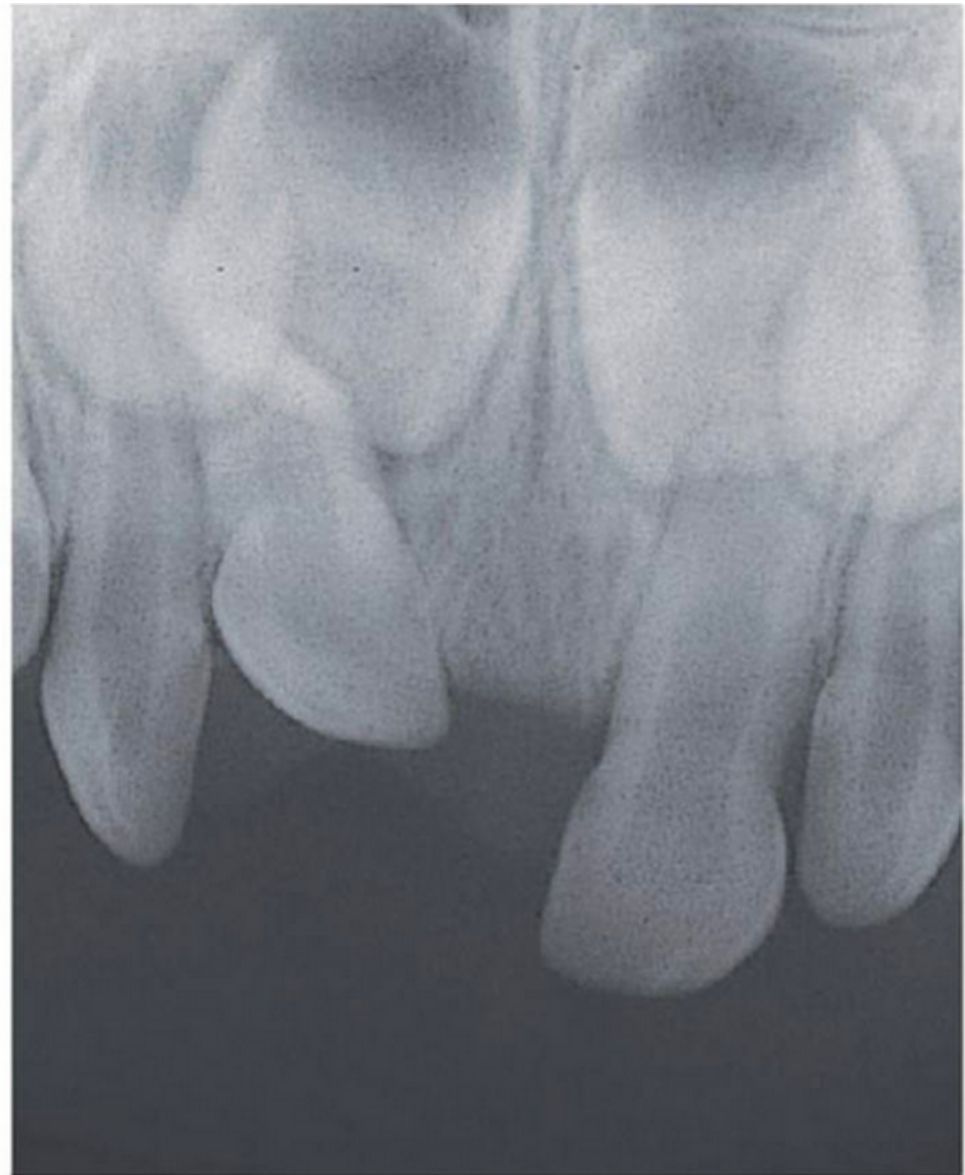
Clinical Case Example13
[
Clinical References for Case Management14
Spontaneous Re-eruption Case
A child presented with teeth 51 and 61 nearly 90% intruded. A conservative “wait and see” approach was taken. Six months later, the teeth had spontaneously re-erupted. Long-term monitoring remained necessary due to the 1-in-3 risk of late-stage complications.
 |  |
- Lauridsen et al. 2017
- Koch et al. 2017
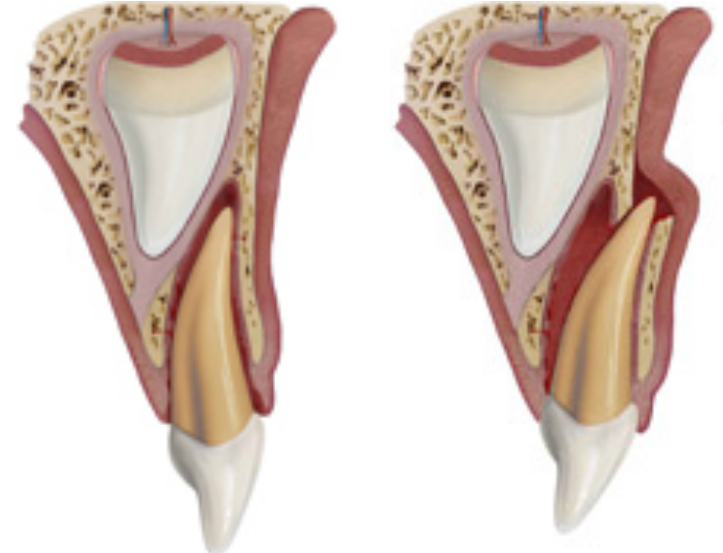
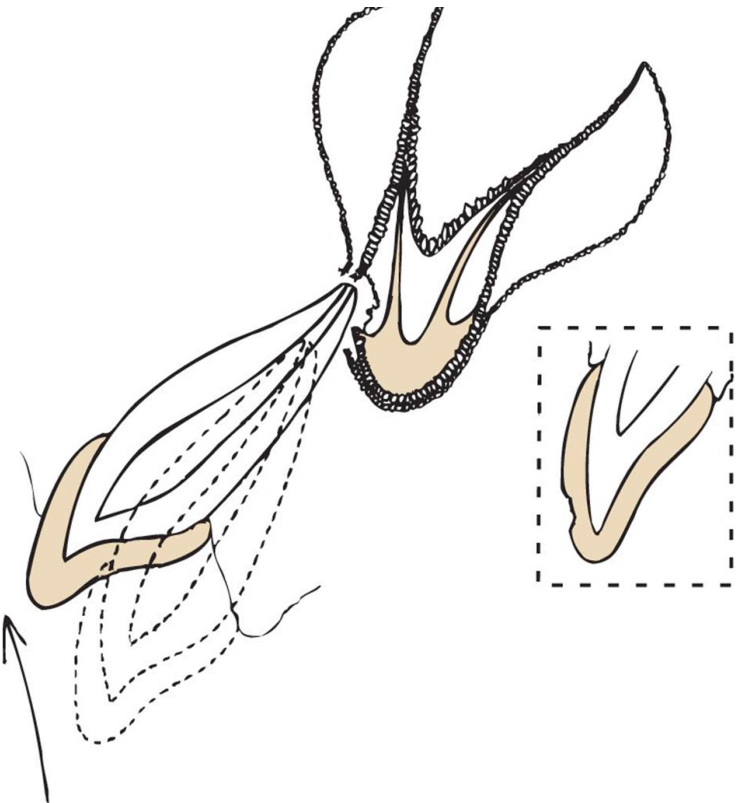
Buccal vs. Palatal Displacement
If the root is pushed buccally (away from the permanent tooth), the prognosis for the permanent successor is better. If pushed palatally (toward the follicle), the risk of damage is high. -
 |  |
 |  |
Extrusive and Lateral Luxation15
-
Complication Rates:
- Extrusion: 15–43%
- Lateral Luxation: 20–40%
-
Types of Complications: Pulp necrosis, resorption, PCO, and premature tooth loss.
-
Prognostic Factors (Lauridsen et al. 2017):
- 96% of complications occur within the first 12 months.
- Higher risk in children over 4 years of age or when a concomitant crown fracture is present.
Extraction Indications
Indications for Extraction vs. Conservative Care16
Extraction is preferred over conservative management (soft diet/monitoring) when the following are present (Andersson et al. 2012):
- Severe extent of injury.
- Occlusal interference that prevents normal closing.
- Direct pulpal exposure.
- Degloving injuries.
Management of Crown Fractures
Management Protocols by Fracture Type17
-
Severe displacement (e.g., severe extrusion or root pushed into the permanent tooth follicle).
-
Infection or evidence of necrosis/abscess.
-
Laterally luxated tooth preventing the child from biting together (specific indication).
-
Uncomplicated Crown Fractures:
- Managed via conservative treatment and regular clinical review.
- Specifically, smooth sharp edges or restore with composite.
-
Complicated Crown Fractures:
- Extraction is the standard treatment.
- Referral to a paediatric dentist may be considered if parents wish to explore specialized options to maintain the tooth.
Root Fractures
- Usually require extraction if the coronal fragment is highly mobile.

Complications of Dental Trauma
Common Post-Traumatic Sequelae18
- Pulp necrosis
- Pulp canal obliteration (PCO)
- Tooth discolouration
- Ankylosis
- Gingival defects
- Premature tooth loss
- Root resorption
Frequency and Clinical Characteristics
- Pulp necrosis occurs in approximately 25% of cases.
- Pulp canal obliteration involves the canal filling with calcified tissue, causing the tooth to turn yellow.
- Tooth discoloration occurs in approximately 52% of cases.
- Ankylosis involves fusion of the tooth to the bone, leading to infra-occlusion and inhibition of alveolar growth.
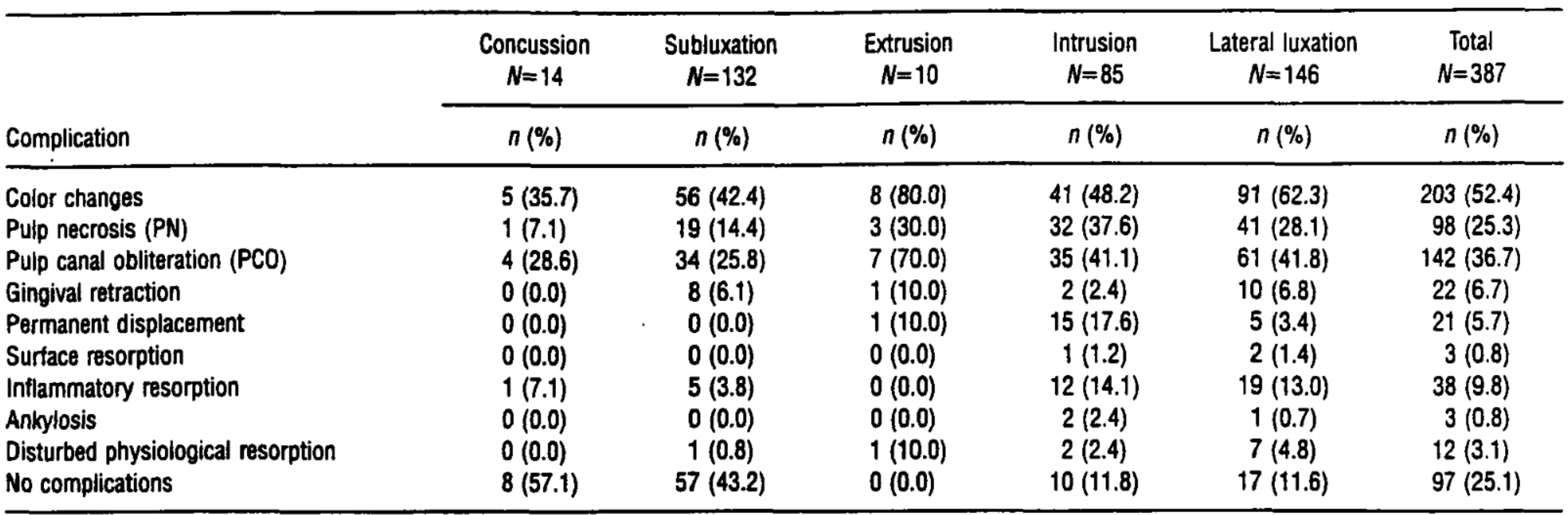
Frequency and Types of Complications
Complication Frequencies by Luxation Type (Borum & Andreasen)19
Data based on 387 traumatized primary teeth:
- Color Changes: Highest in Extrusion (80.0%) and Lateral Luxation (62.3%).
- Pulp Necrosis (PN): Highest in Intrusion (37.6%) and Extrusion (30.0%).
- Pulp Canal Obliteration (PCO): Highest in Extrusion (70.0%) and Lateral Luxation (41.8%).
- Inflammatory Resorption: Most frequent in Intrusion (14.1%) and Lateral Luxation (13.0%).
- Permanent Displacement: Seen primarily in Intrusion (17.6%).
- No Complications: Most common in Concussion (57.1%) and Subluxation (43.2%); 0% for Extrusion cases
Color Change Interpretation
While color change is the most common complication overall (~50%), it is critical to note that discoloration does not always indicate pulp necrosis. A tooth may be discolored yet remain asymptomatic and healthy. .
Case Study: Intrusion and Long-term Review
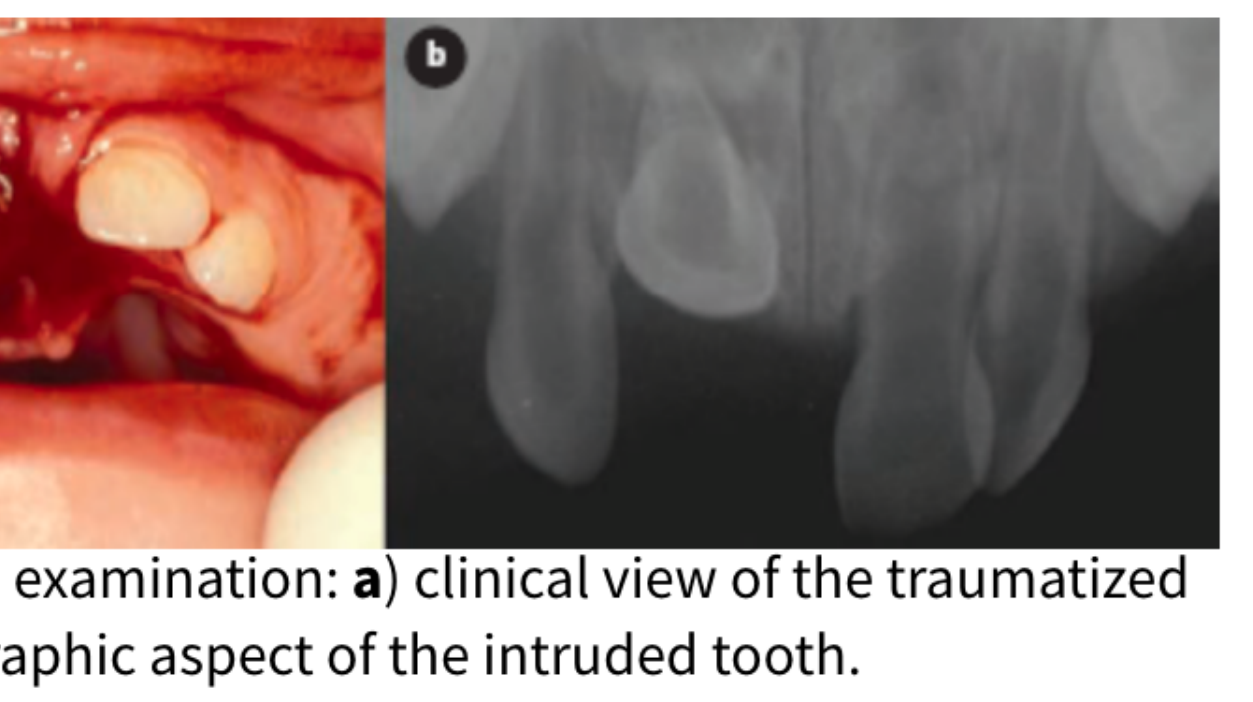
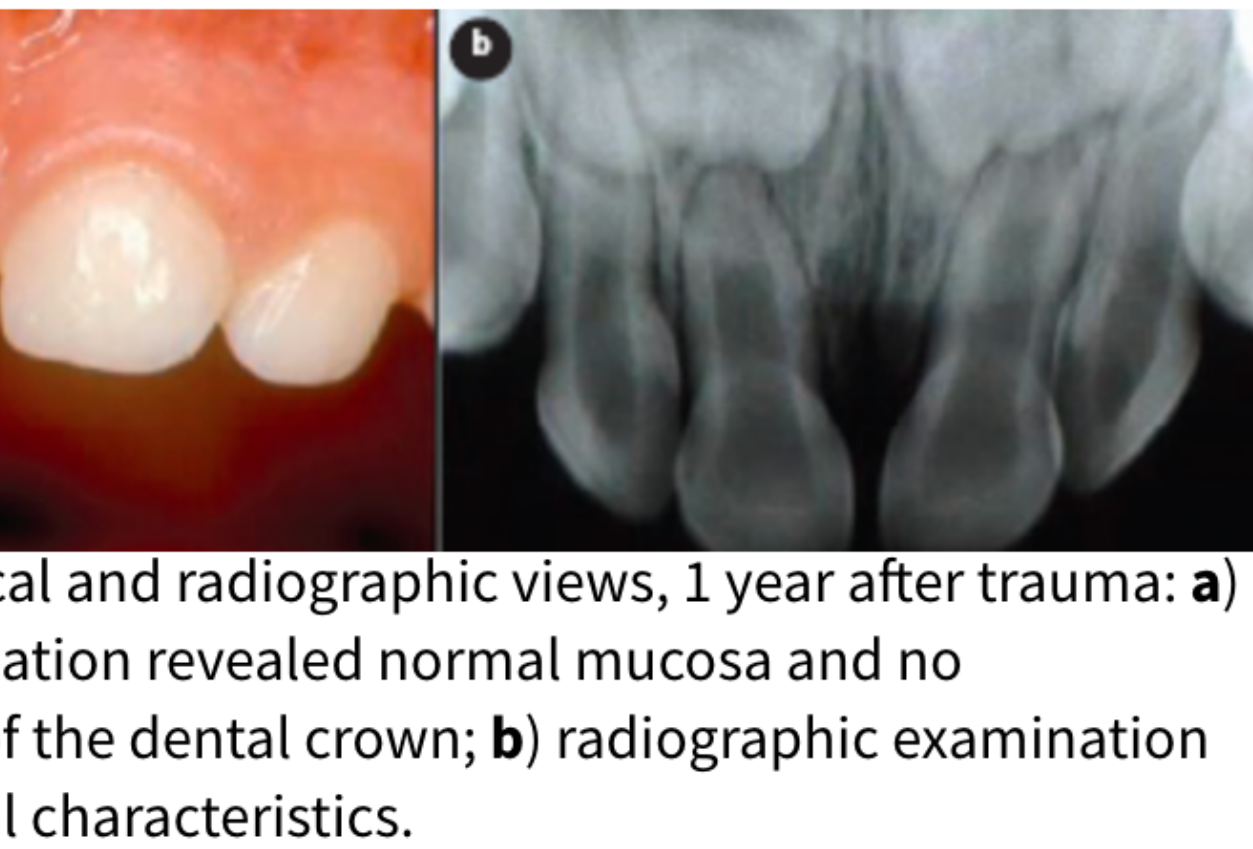
Initial Presentation and 12-Month Review20
- Patient: 14-month-old boy.
- Injury: Tooth 51 intrusive and palatal luxation.
- Treatment: Repositioned under local anaesthesia (LA).
- 1-Year Follow-up: Clinical examination showed normal mucosa and no crown discolouration. Radiographs showed normal characteristics (Gomes et al. 2010).
 |  |
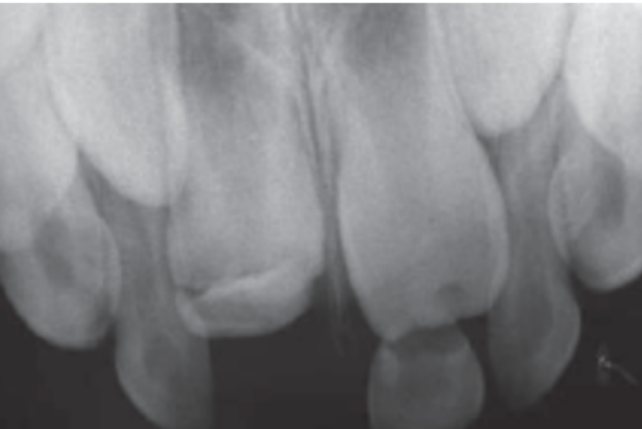
4-Year Review: Long-term Sequelae21
- Radiographic Findings: Signs of alteration in the germ of the maxillary right central permanent incisor.
- Permanent Tooth Malformations:
- Enamel hypoplasia on the permanent maxillary right central incisor.
- Circular enamel hypoplasia on the permanent left central incisor.
- Dilaceration and discoloration of the crown of tooth 11 (Gomes et al. 2010).
Summary of 4-Year Review Findings22
- Developmental Impact: Radiographic evidence of trauma-induced alterations to the permanent successor germ.
- Clinical Presentation of Permanent Teeth:
- Enamel hypoplasia (maxillary right central incisor).
- Circular enamel hypoplasia (left central incisor).
- Discoloration of tooth 11 and isolation issues with tooth 21 (Gomes et al. 2010).
Risks of Repositioning
This case highlights why repositioning is discouraged in primary tooth intrusion. The act of repositioning likely forced the primary root or an inflammatory clot into the permanent tooth germ, causing permanent developmental damage that is extremely difficult to treat later.
 |  |
 |
Recommended Reading and References readings
Clinical Resources and Guidelines23
- Dental Trauma Guide
- International Association of Dental Traumatology (IADT) Guidelines
- Andersson L, Andreasen JO, Day P. Guidelines for the Management of Traumatic Dental Injuries: 3. Injuries in the Primary Dentition. Dental Traumatology 2012; 28: 174-182.
- ==Borum and Andreasen: Classic study on complications and color changes in traumatized primary teeth.==
Footnotes
-
Original PDF page 1: L8 Dental Trauma Primary Dentition, p.1 ↩
-
Original PDF page 2: L8 Dental Trauma Primary Dentition, p.2 ↩
-
Original PDF page 3: L8 Dental Trauma Primary Dentition, p.3 ↩
-
Original PDF page 4: L8 Dental Trauma Primary Dentition, p.4 ↩
-
Original PDF page 5: L8 Dental Trauma Primary Dentition, p.5 ↩
-
Original PDF page 6: L8 Dental Trauma Primary Dentition, p.6 ↩
-
Original PDF page 7: L8 Dental Trauma Primary Dentition, p.7 ↩
-
Original PDF page 8: L8 Dental Trauma Primary Dentition, p.8 ↩
-
Original PDF page 9: L8 Dental Trauma Primary Dentition, p.9 ↩
-
Original PDF page 10: L8 Dental Trauma Primary Dentition, p.10 ↩
-
Original PDF page 11: L8 Dental Trauma Primary Dentition, p.11 ↩
-
Original PDF page 12: L8 Dental Trauma Primary Dentition, p.12 ↩
-
Original PDF page 13: L8 Dental Trauma Primary Dentition, p.13 ↩
-
Original PDF page 14: L8 Dental Trauma Primary Dentition, p.14 ↩
-
Original PDF page 15: L8 Dental Trauma Primary Dentition, p.15 ↩
-
Original PDF page 16: L8 Dental Trauma Primary Dentition, p.16 ↩
-
Original PDF page 17: L8 Dental Trauma Primary Dentition, p.17 ↩
-
Original PDF page 18: L8 Dental Trauma Primary Dentition, p.18 ↩
-
Original PDF page 19: L8 Dental Trauma Primary Dentition, p.19 ↩
-
Original PDF page 20: L8 Dental Trauma Primary Dentition, p.20 ↩
-
Original PDF page 21: L8 Dental Trauma Primary Dentition, p.21 ↩
-
Original PDF page 22: L8 Dental Trauma Primary Dentition, p.22 ↩
-
Original PDF page 23: L8 Dental Trauma Primary Dentition, p.23 ↩