Periodontal Therapy Procedures and Wound Healing
Biological Principles of Periodontal Healing1
The success of periodontal therapy depends on the body’s ability to repair or regenerate tissues lost to disease. Understanding the cellular and molecular mechanisms of wound healing is essential for selecting appropriate surgical and non-surgical interventions.
Types of Periodontal Repair
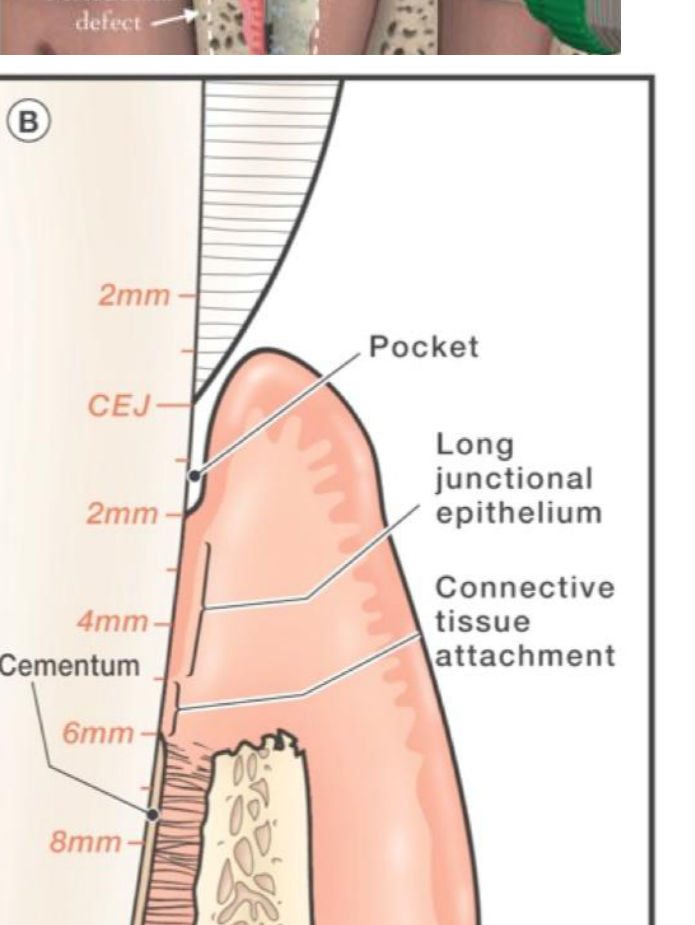
- Repair: Healing by tissue that does not fully restore the architecture or function of the part. An example is the formation of a long junctional epithelium.
- New Attachment: The union of connective tissue or epithelium with a root surface that has been deprived of its original attachment apparatus.
- Regeneration: The reproduction or reconstitution of a lost or injured part. In periodontics, this specifically refers to the restoration of lost cementum, periodontal ligament, and alveolar bone.
- Reattachment: The reunion of epithelial and connective tissue with a root surface after separation by incision or injury, but not by disease.
Factors Influencing Wound Healing
- Local Factors
- Plaque control and oral hygiene
- Mechanical trauma
- Smoking and tobacco use
- Localized infection
- Systemic Factors
- Diabetes mellitus and other metabolic disorders
- Nutritional deficiencies (e.g., Vitamin C)
- Immunosuppressive medications or conditions
- Age and general health status
Clinical Objectives of Therapy
- Elimination of gingival inflammation and correction of conditions that cause it.
- Reduction or elimination of periodontal pockets.
- Establishment of a stable, functional periodontal attachment.
- Creation of an oral environment that the patient can maintain through effective home care.
Reading Resources
Required Textbook Readings2
- Lindhe’s Clinical Periodontology and Implant Dentistry (Volume 7, 2022)
- Chapter 21: Periodontal Wound Healing
- Chapter 45: Periodontal Regeneration
Supplemental Video Resources
Aims of Periodontal Therapy3
- Restore and maintain structure and function of teeth throughout the individuals’ life.
- Control dysbiosis, inducing favourable clinical alterations in the periodontium.
- Regeneration / repair.
- Improve aesthetics.
Overview of Periodontal Procedures
Non-Surgical and Surgical Interventions4
- Non–surgical therapy after risk factor management (steps 1 and 2)
- Following scaling and root planing (debridement), a pocket may reduce from 6mm to 3mm, healing via the formation of a Long Junctional Epithelium (LJE).
- Surgical
- Surgical therapy (mucoperiosteal flap)
- Full Thickness (Muco-periosteal) Flap: The incision touches the bone, and the periosteum is reflected with the soft tissue; typically used for regenerative procedures like GTR.
- Partial Thickness (Mucosal) Flap: The periosteum is left on the bone; only the mucosa is reflected.
- Common flap shapes include triangular and trapezoidal designs.
- Regenerative procedures, guided tissue/ bone regeneration
- Periodontal plastic / pre-prosthetic surgery
- Implant surgery
- Surgical therapy (mucoperiosteal flap)
Advanced and Adjunctive Therapies
- Growth factors
- Cell therapy
- Gene therapy
- 3D printed scaffolds
- Host modulation therapy (e.g., NSAID, low dose tetracyclines) to control enzymes
- Bone metabolism enzyme control
- Antioxidants (e.g., resveratrol)
Biological Principles of Wound Healing
Peculiarities in the Periodontal Area5
- Wound margins are opposing a rigid non-vascularized surface.
- After non-surgical periodontal therapy, the pocket heals by forming long junctional epithelium.
 |  |
Definitions of Wound and Healing
Wound/Injury
Disruption of the anatomic structure and function in a body part.
Healing
Cell/tissue response to injury in an attempt to restore the normal structure and function.
Phases of Wound Healing
Early and Late Phases6
Healing involves a sequence of well-orchestrated innate temporal and spatial events that dictate the outcomes of wound healing, either periodontal regeneration or periodontal repair.

Biological Processes
These events follow a dynamic complex biomolecular path involving:
- Cell migration
- Proliferation
- Differentiation
- Angiogenesis
- Extracellular matrix formation and remodeling
Immediate Response7
- Initial clot: Essential to protect the wound and act as a matrix for cell migration.
Hemostasis and Dry Socket
Clot formation is the critical first step. If a clot does not form or is dislodged (e.g., via negative pressure from using a straw after extraction), it leads to a dry socket. Treatment involves irrigating, curetting to induce bleeding, and forming a new clot.
Inflammation Phase
- Growth factors in the initial blood clot attract inflammatory cells (mostly neutrophils and monocytes) which cleanse the wound and initiate repair.
Granulation Phase (Approx. Day 4)
- Macrophages predominate to continue decontamination.
- Formation of granulation tissue with recruitment of fibroblasts, endothelial cells, and smooth muscle cells.
- Granulation tissue consists of new blood vessels, connective tissue fibers, and fibroblasts.
- Highly regulated process involving growth factors and cytokines.
- Collagen formation and cell-matrix/cell-to-cell links occur.
Maturation Phase (Approx. Day 7)
- Fibroblasts aid in tissue maturation.
- By day 7, fibroblasts occupy the site, and tissue remodeling follows the initial tissue formation.
- Myofibroblasts help wound contraction.
- Healing responds to functional demands (regeneration or repair).
Factors Affecting Healing
- Local factors: Infection, tissue trauma, poor vascular perfusion.
- Systemic factors: Hormones, stress, nutritional deficiencies.
Comparison
Periodontal wound healing is more complex than epidermal wound healing.
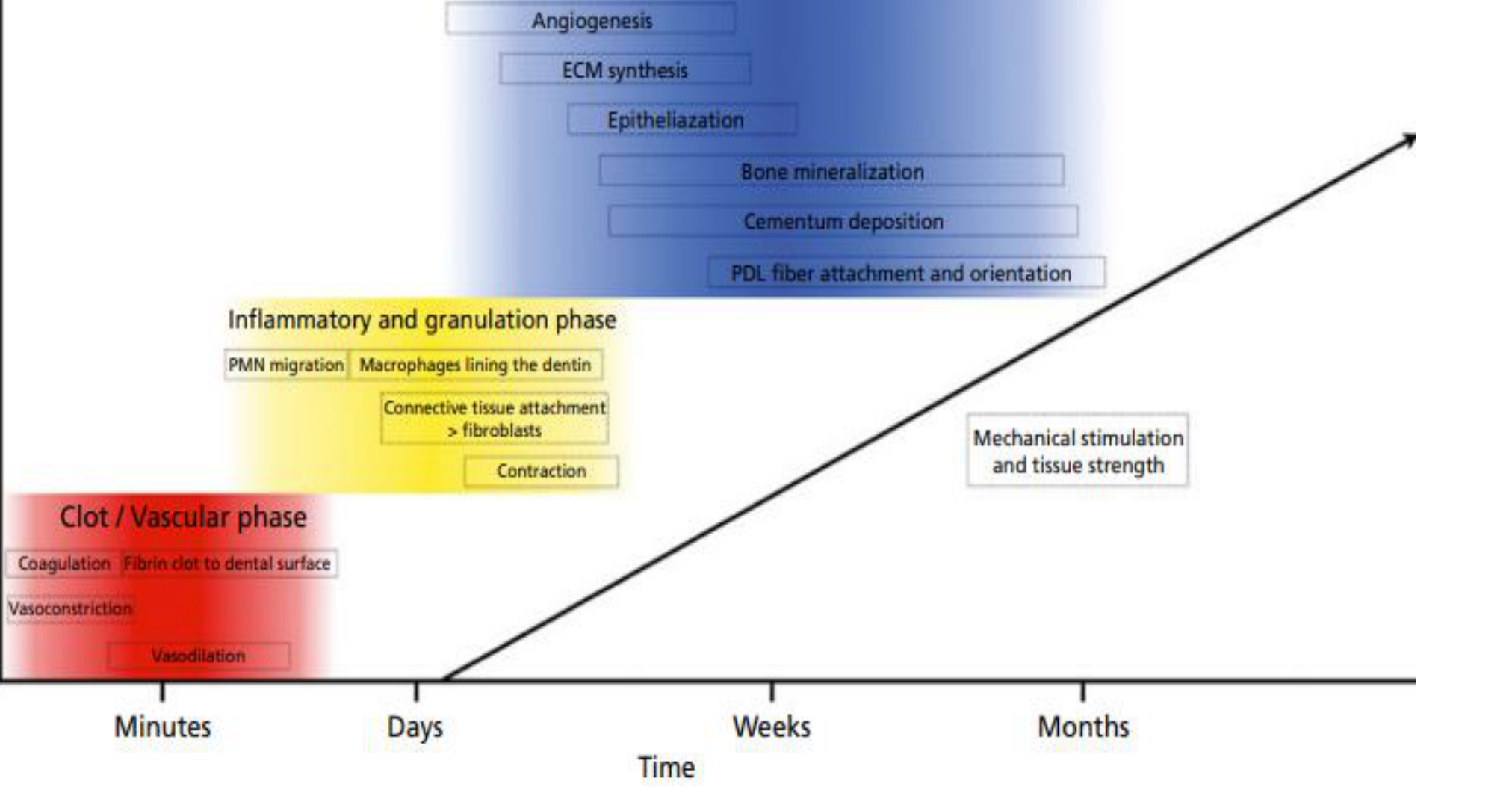
Timeline of Healing Events8
-
Clot / Vascular Phase (Minutes)
- Vasoconstriction
- Coagulation: Fibrin clot to dental surface
- Vasodilation
-
Inflammatory and Granulation Phase (Days)
- PMN migration
- Macrophages lining the dentin
- Connective tissue attachment (fibroblasts)
- Contraction
-
Periodontal Regeneration (Weeks)
- Angiogenesis
- ECM synthesis
- Epithelialization
- Bone mineralization
- Cementum deposition
- PDL fiber attachment and orientation
-
Periodontal Remodeling and Stability (Months)
- Maturation and remodeling
- Mechanical stimulation and tissue strength
Healing by Primary and Secondary Intention
Healing by First Intention9
Involves wound edges being brought together using sutures. Associated with minimal tissue loss; regeneration predominates over fibrosis. - Occurs when wound edges are approximated and joined by sutures, such as following a surgical incision.
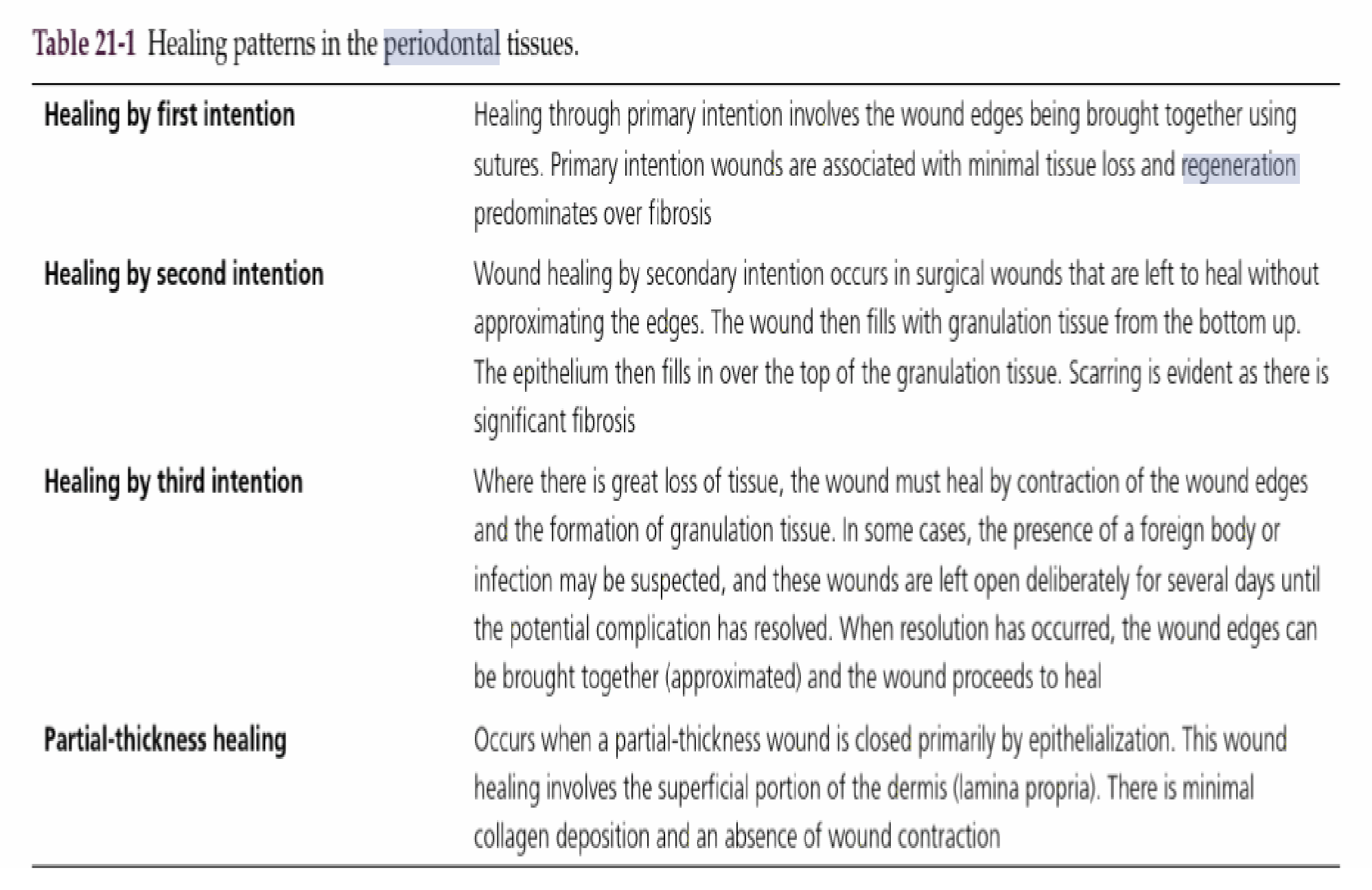
Healing by Second Intention
Occurs in surgical wounds left to heal without approximating edges. The wound fills with granulation tissue from the bottom up, followed by epithelial coverage. Significant fibrosis and scarring are evident. - Examples include a tooth extraction socket left open or a donor site on the palate after a graft. Healing happens as cells migrate from the edges to form epithelium and connective tissue.
Healing by Third Intention
Occurs where there is great loss of tissue; the wound heals by contraction and granulation. Often used when infection or foreign bodies are suspected; wounds are left open for several days before edges are approximated. - Edges may be approximated at a later date if healing is not progressing properly.
Partial-Thickness Healing
Occurs when a wound is closed primarily by epithelialization involving the superficial portion of the dermis (lamina propria). Characterized by minimal collagen deposition and absence of wound contraction.
Outcomes of Periodontal Healing
Clinical Healing Terms10
- Reattachment: Refers to the reattachment of the gingiva to areas from which it was mechanically removed.
- Example: The reunion of epithelial or connective tissue to a root surface after a gingivectomy.
- New attachment: Occurs when newly generated fibers are embedded in new cementum on a portion of the root that was uncovered by disease.
- Resorption: Loss or blunting of some portion of a root; can be idiopathic or associated with inflammation, trauma, or orthodontics.
- Ankylosis: Fusion of the tooth and the alveolar bone.

Repair Versus Regeneration
Repair
Healing of a wound by tissue that does not fully restore the architecture or function. In periodontics, it refers to restoration of a normal gingival sulcus at the same level as the base of the previous pocket. Often typified by a long junctional epithelium.
- Repair can occur after injury from over-probing with more than 25g of force.
- Long Junctional Epithelium (LJE) is considered a weak attachment.
Regeneration
Reproduction or reconstruction of a lost or injured part such that architecture and function are completely restored. This occurs via precursor cells replacing lost tissue.
Regenerative Procedures in Periodontology11
Procedures specifically designed to restore parts of the tooth-supporting apparatus lost due to periodontitis.
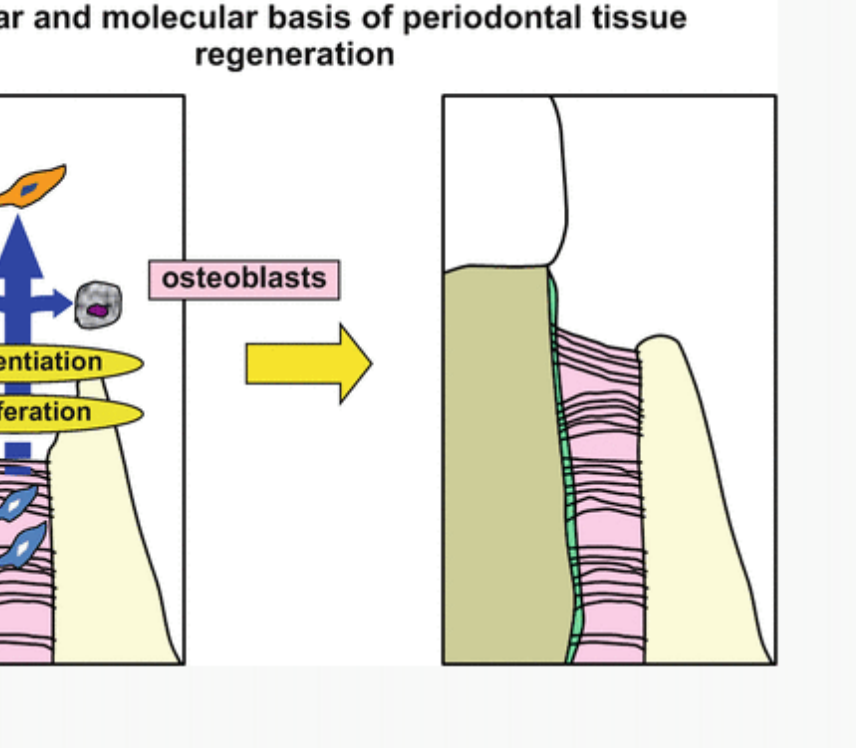
Cellular and Molecular Basis
Periodontal tissue stem cells, including undifferentiated mesenchymal stem cells, are present in the periodontal ligament. Regeneration is achieved by activating these cells to:
- Proliferate
- Migrate
- Site-specifically differentiate at the site of tissue loss
Definition of Regeneration12
Reproduction or reconstruction of a lost or injured part in such a way that the architecture and function of the lost or injured tissues are completely restored. This includes:
- New cementum with inserting and functionally orientated ligament fibers
- Alveolar bone
- Gingiva

Outcomes of Repair13
Healing of injuries without the complete restoration of structure or function of a part.
- Long junctional epithelium: Considered a satisfactory healing result.
- Root resorption: Unsatisfactory outcome.
- Ankylosis: Unsatisfactory outcome.
- Ankylosis prevents the tooth from being moved orthodontically.

Cellular Dynamics and Tissue Repopulation
The Melcher Hypothesis (1976)14
“The type of cell which repopulates the root surface after periodontal surgery determines the nature of the healing that will occur.”
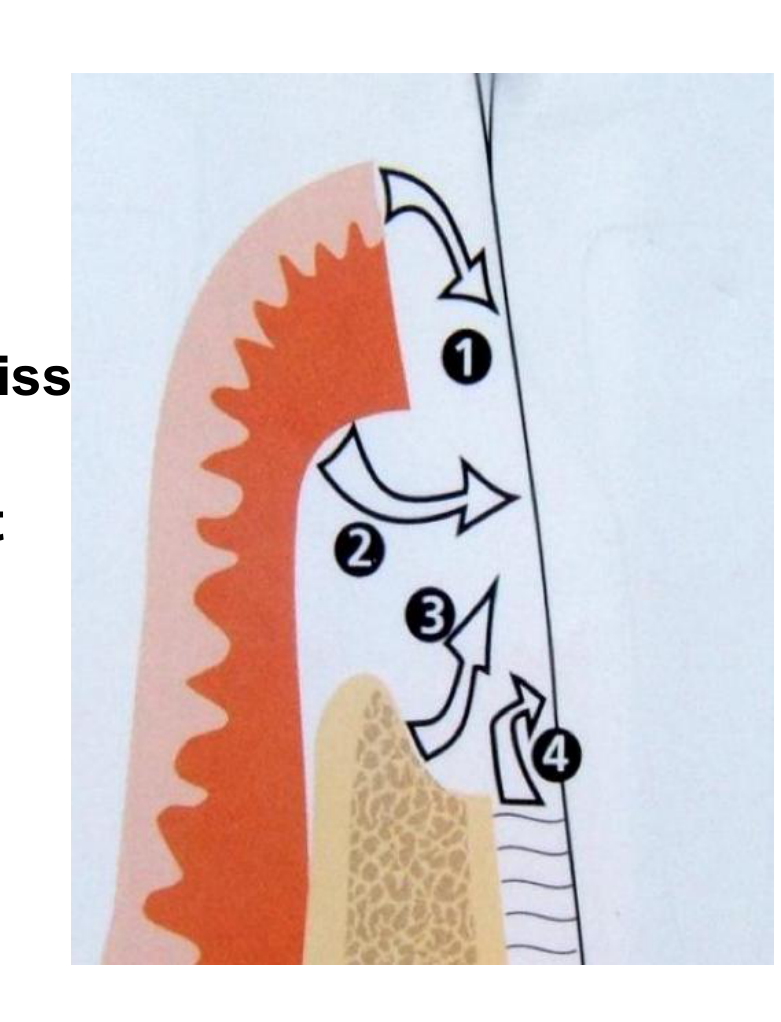
Potential Repopulating Cell Sources
- Epithelium
- Cells derived from the gingival connective tissue
- Cells derived from the alveolar bone
- Cells derived from the periodontal ligament
These cell types possess different embryonic origins and different rates of proliferation.
Migration Rates
Epithelial cells have the highest migration rate (4–7 days), while fibroblasts and osteoblasts take much longer (3–6 weeks). Because epithelial cells are the fastest, they typically form the LJE unless blocked.
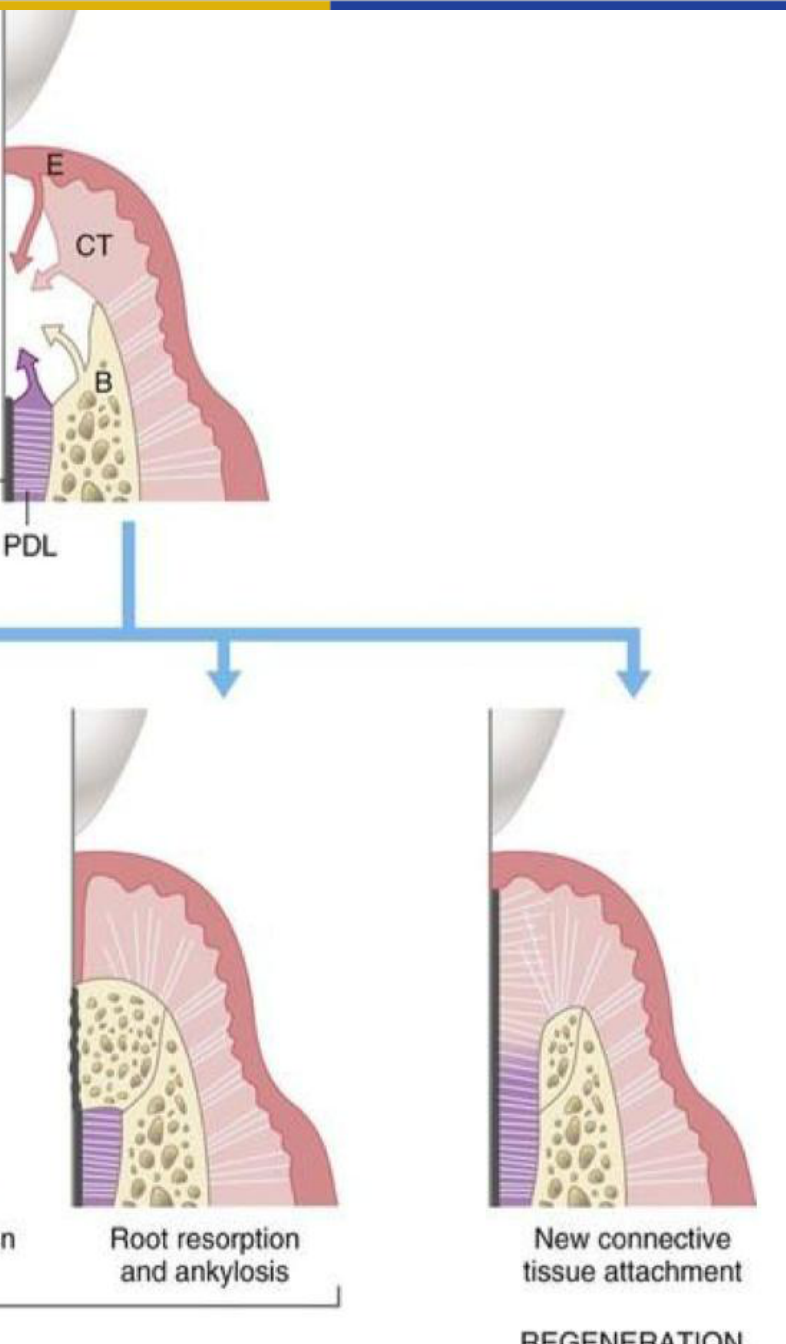
Tissue Source and Healing Outcome15
- Epithelium (E): Results in Long junctional epithelium (Repair).
- Connective Tissue (CT): Results in Connective tissue adhesion and root resorption (Repair).
- Alveolar Bone (B): Results in Root resorption and ankylosis (Repair).
- Periodontal Ligament (PDL) / Cementum: Results in New connective tissue attachment (Regeneration).
 |  |
Healing Potential of Different Tissues
Epithelium16
- Proliferation Speed: Fastest tissue to proliferate; usually “wins the race” to repopulate the wound.
- Outcome: Formation of a long junctional epithelium.
- Function: Primary function is wound coverage and protection against microbes.
- Origin: Ectodermal.
- Clinical Note: To stop epithelium from proliferating and preventing other cell types from reaching the root, Guided Tissue Regeneration (GTR) membranes are used.
Gingival Connective Tissue17
- Origin: Mesodermal.
- Proliferation Speed: Second fastest tissue.
- Outcomes: Connective tissue adhesions, reduction in tissue volume, recession, and root resorption.
Alveolar Bone
- Origin: Mesodermal.
- Outcomes: Ankylosis and resorption.
Periodontal Ligament (PDL)18
- Origin: Ectomesenchymal.
- Significance: The only tissue able to regenerate (Karring et al., 1985).
Key Requirements for Regeneration19
- Wound stability
- Space-provision

Factors Affecting Regeneration Potential
Categories of Influence20
- Patient factors
- Defect factors
- Tooth factors (e.g., restorability, mobility)
- Surgical factors
Patient and Defect Factors
Patient Factors and Controllability21
- Local Factors:
- Plaque (Full Mouth Plaque Score <15%)
- Infection (Full Mouth Bleeding Score <15%)
- Behavioral Factors:
- Smoking (>10 cigarettes/day)
- Compliance
- Systemic Factors:
- Stress
- Diseases (e.g., diabetes)
- Diabetes must be controlled.
- Patients on bisphosphonates (e.g., Prolia) require extreme caution due to the risk of necrosis.
- Cultural Sensitivity: Patients may refuse certain grafts (e.g., bovine or cadaver-derived) based on religious or personal beliefs.
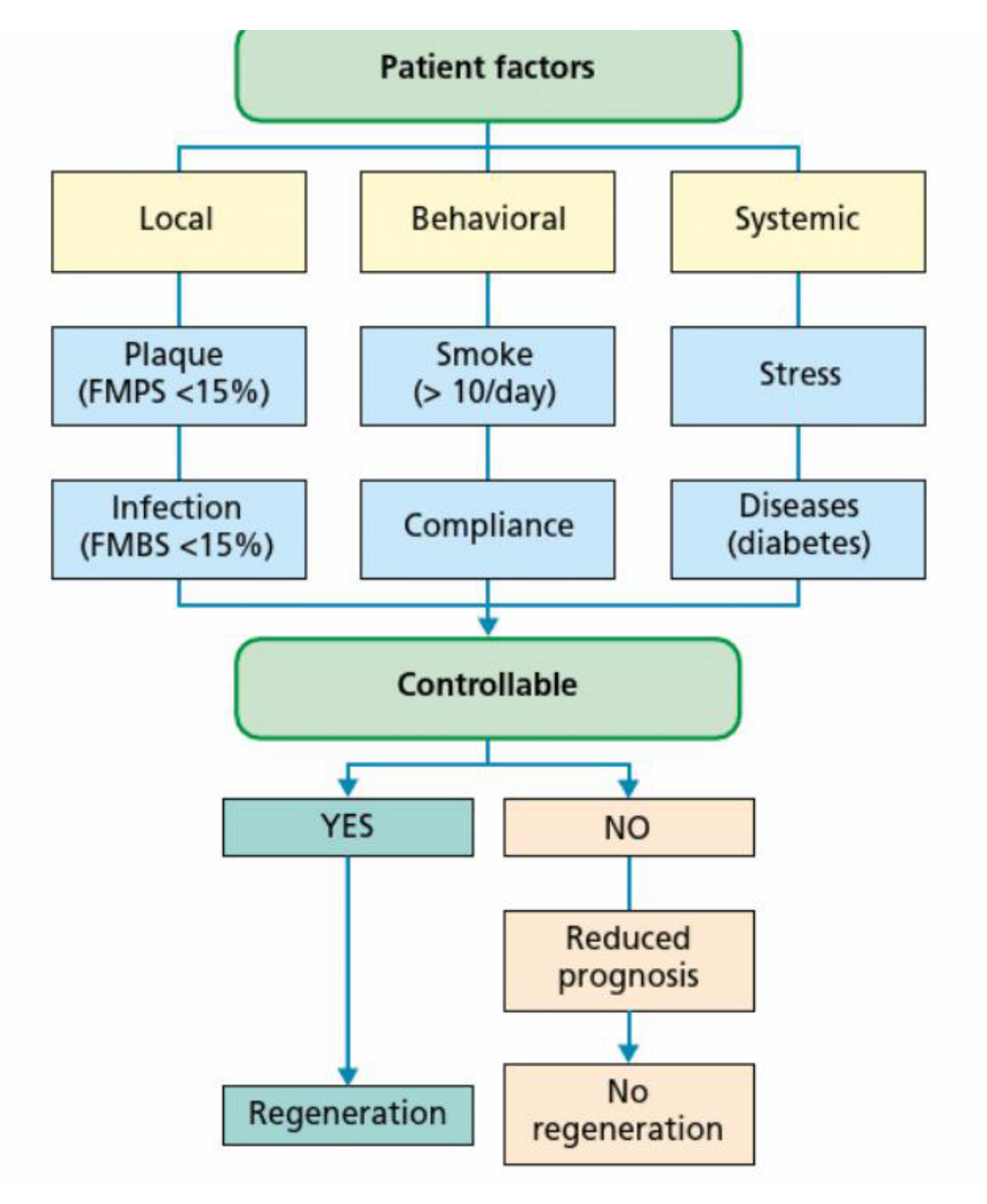
Prognostic Impact
- Controllable (Yes): Regeneration is possible.
- Not Controllable (No): Reduced prognosis; regeneration is unlikely.
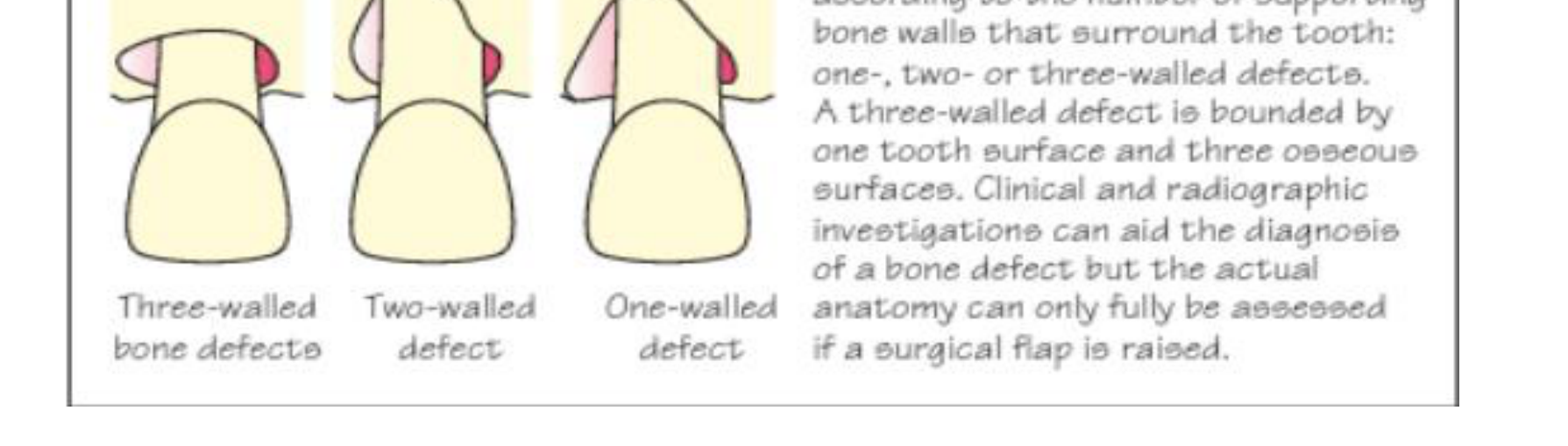
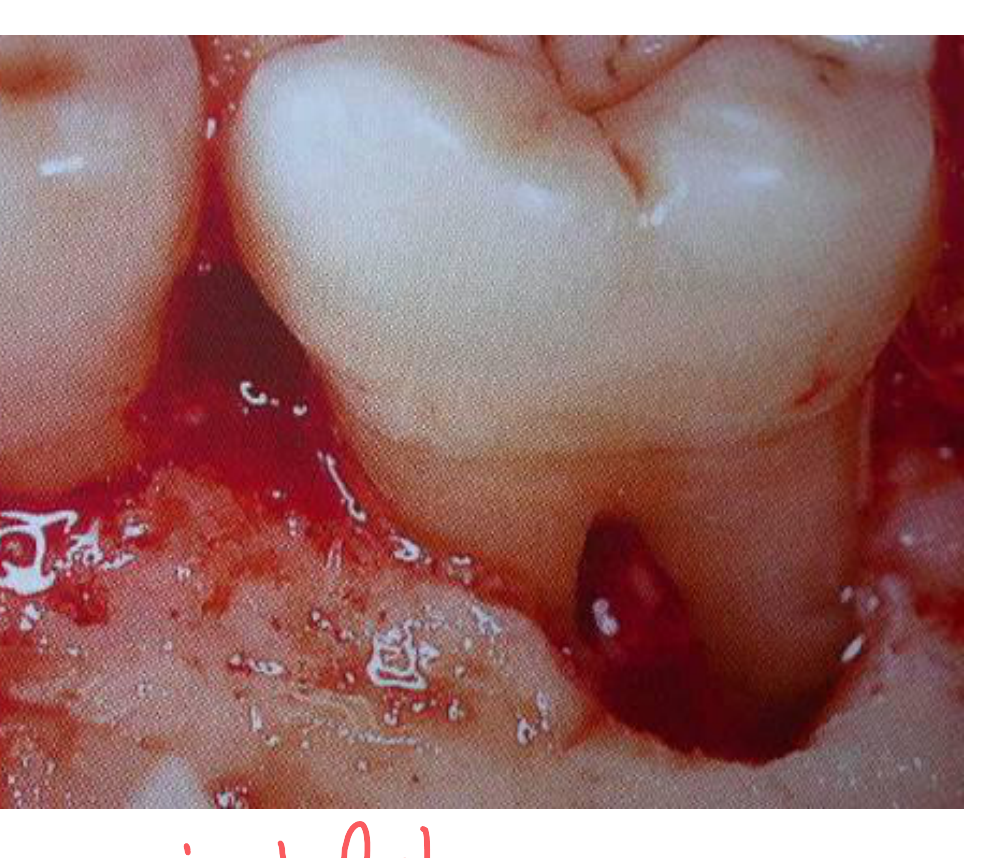
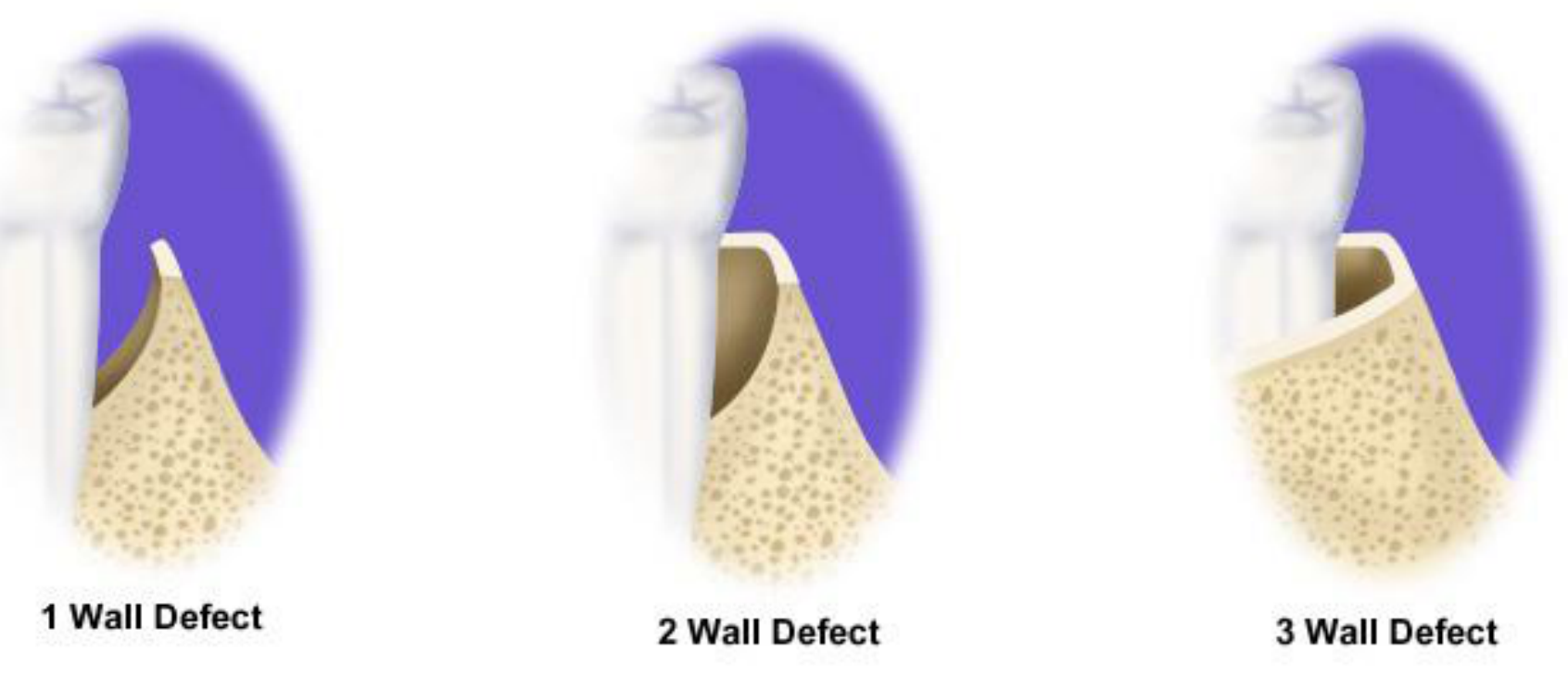
Defect Characteristics22
- Bony Defect Size: Ideally 3 or 4 walls.
- Three-wall defect: Three walls present, one absent (Best prognosis).
- Two-wall defect: Two walls present, two absent (Most common; also called a "crater").
- One-wall defect: One wall present, three absent.
- Depth: Minimum 3mm.
- Width: Narrow defects are preferred.
- Contained vs. Non-contained: Bone grafts require a "contained" space (like an angular/infrabony defect) to stay in place; they cannot easily be used in horizontal bone loss.
- Surrounding Soft Tissue: Sufficient, thick, and keratinized tissue is ideal.
- Accessibility: Ease of surgical access.
Clinical Decision Tree for Intrabony Defects
Assessment and Initial Decision (A & B)23
- Assess Intrabony Defect: Evaluate PD, CAL, BOP, mobility, osseous architecture, and systemic/behavioral issues.
- Determine Defect Depth: If depth is <3 mm, consider non-surgical management or osseous surgery with resection based on PD and patient factors.
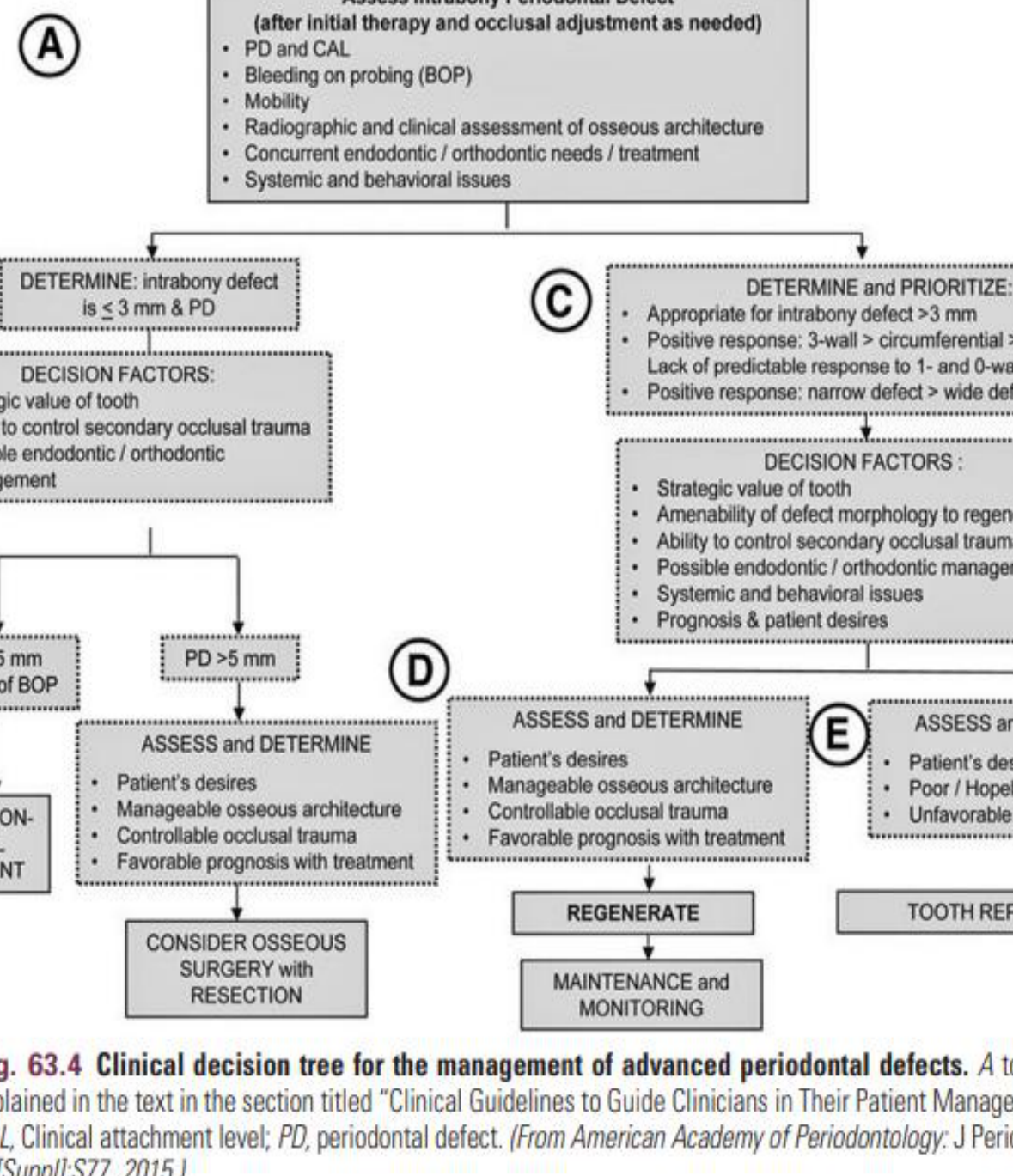
Prioritizing Regeneration (C & D)
- Favorable Morphology: 3-wall > circumferential > 2-wall defects; narrow > wide defects.
- Decision Factors: Strategic value of tooth, ability to control trauma, and patient desires.
- Outcome: If favorable, proceed to Regenerate, followed by maintenance and monitoring.
Tooth Replacement (E)
- Criteria: Poor/hopeless prognosis, unfavorable endodontic status, or patient preference for replacement.
Surgical and Technical Factors
Critical Surgical Elements24
- Blood supply
- Clot stabilization
- Wound coverage
- Surgical technique
- Space maintenance

Clinical Methods to Promote Regeneration
Physical Methods25
- Bone grafts
- Barrier devices or membranes for Guided Tissue Regeneration (GTR)
- 3D printed scaffolds
Biochemical Methods
- Extracellular matrix and growth factors (experimental)
- Enamel matrix proteins (e.g., Emdogain)
Clinical vs. Histological Success
Clinically, some cases appear successful, but histologically an epithelial lining may be present against bone instead of new cementum and bone.
Bone Grafts and Substitutes
Types of Bone Grafts26
Biological Mechanisms of Grafts
- ==Osteogenesis: Potential to form bone via viable cells.==
- ==Osseoinduction: Chemical stimulation of bone formation.==
- ==Osseoconduction: Physical scaffold for bone growth.==
- Autogenous bone: From the same patient.
- ==Best because it is osteogenic (contains live cells).==
- ==Isograft: Taken from identical twins.==
- Bone derivatives:
- Allogeneic: From the same species (another human).
- ==Taken from a cadaver; it is osteoinductive.==
- Xenogeneic: From a different species (bovine, equine, porcine).
- ==These materials are osteoconductive.==
- Bone substitutes: Synthetic biomaterials.
- Synthetic/factory-manufactured material.
Limitations
- There is limited evidence of histological regeneration if no membrane is used to exclude epithelium/connective tissue.
- These materials often act as a “biological obturation” or filling of the defect rather than inducing true regeneration.
Scaffold Materials for Oral Tissue Engineering27
- Allografts:
- Demineralized freeze-dried bone allograft (DFDBA)
- Freeze-dried bone allograft (FDBA)
- Xenografts:
- Anorganic bovine bone (e.g., Bio-Oss, OsteoGraf, Pep-Gen P-15)
- Hydroxyapatite (HA)
- Alloplasts (Synthetic):
- Tricalcium phosphate (e.g., Synthograft)
- Hydroxyapatite (e.g., Periograft, Osteogen)
- Bioactive glass polymers (e.g., PerioGlas, BioGran)
- Hard tissue replacement polymer (e.g., Bioplant)
- Coralline calcium carbonate (e.g., Biocoral)
- Polymers and Collagens:
- Collagen (e.g., CollaPlug, CollaCote, Gelfoam)
- Poly(lactide-co-polyglycolide)
- Hyaluronic acid ester

Guided Tissue Regeneration and Membranes
Purpose of Membranes
To act as a physical barrier to stop fast-moving epithelial cells from reaching the root, allowing slower-moving bone and PDL cells to populate the area.
Membrane Types28
- Non-resorbable
- Must be surgically removed later.
- Resorbable
- Dissolve on their own (similar to resorbable sutures).
Challenges Limiting Clinical Results
- Technique sensitivity (microsurgical approaches required)
- Instability and membrane collapsing
- Infection and recession
- Patient factors (biofilm control, smoking)
Management of Degree II Furcation Defect293031
- Repair defect
- Membrane placement
- Flap management
 |  |
 |
Nonresorbable Membranes32
- History: Cellulose acetate filters were used in classic studies; expanded PTFE (ePTFE) became the first commercial standard.
- Properties: ePTFE provides a cellular barrier, is biocompatible, maintains space, permits tissue integration, and is clinically manageable.
- Current Use: While less common for routine GTR, they remain popular for guided bone regeneration and ridge preservation.
Bioresorbable Membranes33
These have largely replaced ePTFE for routine GTR. Types include:
- Polyglycoside synthetic polymers: (e.g., polylactic acid) Degraded by nonenzymatic cleavage into lactic acid and pyruvate.
- Collagen: (e.g., porcine collagen) Degraded by collagenases, gelatinases, and peptidases.
- Calcium sulfate.
Intrabony Defects3435
- Regeneration is more reliable in 3-wall defects compared to 1-wall defects.
- Key to success: Wound stability and space provision.
Enamel Matrix Derivatives
Biological Basis36
- Enamel matrix proteins are active during periodontal embryonic formation.
- EMDOGAIN: Commercially available porcine enamel matrix proteins (mostly amelogenin).

Clinical Advantages
- Shown to affect wound closure, reduce inflammation, and increase predictability.
- Less technique-sensitive than membranes with fewer complications.
- Can be combined with bone grafts and used with minimal surgical procedures.
Clinical Indications for EMD37
-
Intrabony Defects:
- Self-contained: EMD or GTR alone or with bone graft.
- Non-self-contained: EMD or GTR combined with a bone graft.
- Horizontal bone loss: Conventional flap surgery (conservative or resective).
-
Furcation Defects (Class II):
- Mandible: EMD or GTR alone or with bone graft.
- Maxilla: Buccal (EMD/GTR), Mesial (EMD), Distal (Root resection or flap with EMD).
-
Recession Defects:
- Thick biotype: Coronally advanced flap + EMD.
- Thin biotype: Coronally advanced flap + EMD + connective tissue graft (or tunnel technique).

Microsurgical and Flapless Delivery38
- Straumann® Emdogain® FL: Designed for cultivating flapless periodontal regeneration.
- Utilizes a specific delivery system for minimally invasive application.
 |  |
Indications and Contraindications for Emdogain Flapless39
-
Indications:
- Adjunct to non-surgical therapy (initial phase).
- Pockets ≤5mm.
- Implants and wound healing support.
- Good oral hygiene and minimally invasive needs.
-
Contraindications:
- Uncontrolled diabetes or systemic diseases impacting healing.
- Chronic high-dose steroid therapy or metabolic bone disease.
- Radiation/immunosuppressive therapies.
- Infection, vascular impairment, or porcine allergies.
- Smoking.

Step-by-Step Guide for Emdogain Flapless40
- Root Debride and Scale: Removal of biofilm and plaque.
- Root Conditioning: Application of PreGel for 2 minutes to dislodge blood.
- Rinse: Use saline or ultrasonic waterjet.
- Haemostasis: Can be facilitated by packing floss into the pocket.
- Emdogain FL Application: Apply from the pocket base upwards until excess is seen.
- Post-operative Instructions: Include interdental brushing and recall at 2–3 month intervals.
Advanced Technologies and Future Therapies
Cell Therapy41
- Soft Tissue: Autogenous fibroblasts/keratinocytes in Alloderm used for trauma or malignancies (non-self-renewing).
- Bone: Expanding autologous bone marrow-derived stem cells shows promise for alveolar defects.
Gene Therapy
- Experimental potential for producing bioavailable growth factors (e.g., Gen21s for bone formation).
- ==Gem21s (synthetic PDGF - Platelet-Derived Growth Factor) is used to stimulate healing in furcations and recession.==
3D Printed Scaffolds
- Provides space and wound stability.
- Guides complex spatial/temporal interactions.
- Customized biodegradable polymers can be designed from CT images of specific bone defects.
Clinical Applications and Assessment
Primary Indications42
- Furcation defects: Specifically mandibular molar, grade 2, buccal.
- Intrabony defects: Ideally 3-walled, >3mm depth.
- Recession defects.
- Bone regeneration in Implantology.
Indications for Regenerative Therapy
Scaffold Fabrication Methods43
- Prefabricated: Particulated, solid form, or injected.
- Image-based: CT scan of defect followed by rapid prototyping to create a 3D printed scaffold custom-fit to the defect.
- Delivery: Injected or adapted directly into the defect.

Extracellular Matrix and Growth Factors44
- Agents: Fibronectin, PDGF, IGF, TGFs, BMP-3.
- Status: Significant results in animal models, but clinical efficacy is currently insufficient for wide use; high cost.
Other Emerging Techniques
- Systemic Therapies: PTH, sclerostin monoclonal antibody.
- Cell Therapy: Autogenous fibroblasts/keratinocytes for soft tissue loss.
- Stem Cells: Bone marrow-derived stem cells for alveolar bone defects.
Methods of Healing Assessment
Clinical Parameters45
- Gain in clinical attachment levels (CAL).
- Probing depth and bleeding on probing.
Radiological Examination
- Gain in bone levels.
- Checking for bone fill over time (usually takes at least 6 months).
Re-entry Surgeries
- Visual confirmation of bone level gain.
- Occasionally used to visually inspect bone formation.
Histology
- The only definitive way to detect true regeneration.
- Limited by ethical considerations; relies on animal models and indirect evidence from case reports.
Key Lecture Takeaways46
Summary and Case Studies
- Progenitor cells for lost periodontal attachment are only present in the periodontal ligament.
- Regenerative procedures (e.g., GTR and Emdogain) must encourage repopulation by these specific cells.
- Bone grafts typically result in repair rather than regeneration.
- Regeneration is not guaranteed; histology is the only way to confirm it.
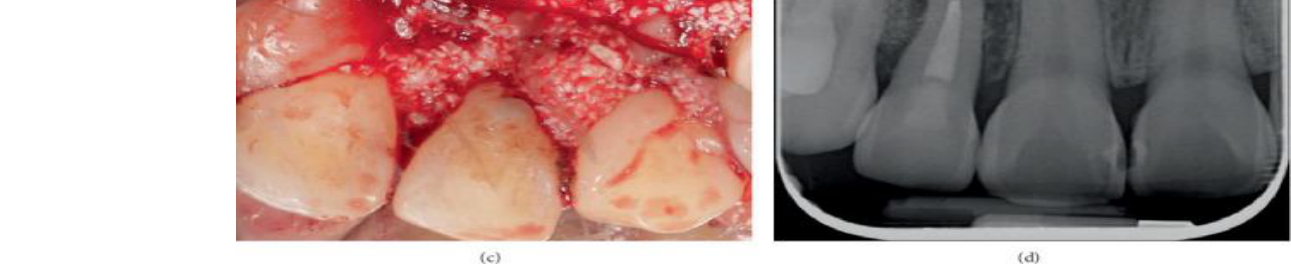
Case Report: Palatoradicular Groove Management47
 |  |  |
 |  |  |
 |
Case: Palatal Root Groove48
- Management of a bone defect caused by a palatal root groove.
- Clinical images (a-d) demonstrating the condition and procedural steps.
Case: Palatal Root Groove Management
- Patient Presentation: Lateral incisor with a deep palato-radicular groove and significant bone loss.
- Endodontic Strategy: Elective root canal treatment is advocated prior to periodontal debridement to prevent pushing bacteria into the canal system.
- Surgical Technique (MAPS): Minimal Access Papilla Space (MAPS) was utilized to avoid circular incisions and prevent "black triangles" in the aesthetic zone.
- Procedure: The groove was smoothed, bone graft placed, and the site closed.
- Outcome: Significant bone formation observed at 6 months, 1 year, and 2 years post-operatively.
Audio Appendix
Additional Audio Content
The following sections from the lecture audio did not correspond to any heading in the main document.
Enamel Matrix Derivatives (e.g., Endogain)
- Biological Basis: A gel used to induce bone and tissue formation.
- Clinical Use: Can be used in infrabony defects, furcations, and recession. It is often combined with bone grafts and GTR membranes for a “triple” effect (Scaffold + Induction + Barrier).
- Root Conditioning: Using “Pre-gel” (EDTA, citric acid, or tetracycline) to remove the smear layer and facilitate better attachment.
 |  |
 |
Footnotes
-
Original PDF page 1: L5 Wound healing and regeneration New, p.1 ↩
-
Original PDF page 2: L5 Wound healing and regeneration New, p.2 ↩
-
Original PDF page 3: L5 Wound healing and regeneration New, p.3 ↩
-
Original PDF page 4: L5 Wound healing and regeneration New, p.4 ↩
-
Original PDF page 5: L5 Wound healing and regeneration New, p.5 ↩
-
Original PDF page 6: L5 Wound healing and regeneration New, p.6 ↩
-
Original PDF page 7: L5 Wound healing and regeneration New, p.7 ↩
-
Original PDF page 8: L5 Wound healing and regeneration New, p.8 ↩
-
Original PDF page 9: L5 Wound healing and regeneration New, p.9 ↩
-
Original PDF page 10: L5 Wound healing and regeneration New, p.10 ↩
-
Original PDF page 11: L5 Wound healing and regeneration New, p.11 ↩
-
Original PDF page 12: L5 Wound healing and regeneration New, p.12 ↩
-
Original PDF page 13: L5 Wound healing and regeneration New, p.13 ↩
-
Original PDF page 14: L5 Wound healing and regeneration New, p.14 ↩
-
Original PDF page 15: L5 Wound healing and regeneration New, p.15 ↩
-
Original PDF page 16: L5 Wound healing and regeneration New, p.16 ↩
-
Original PDF page 17: L5 Wound healing and regeneration New, p.17 ↩
-
Original PDF page 18: L5 Wound healing and regeneration New, p.18 ↩
-
Original PDF page 19: L5 Wound healing and regeneration New, p.19 ↩
-
Original PDF page 20: L5 Wound healing and regeneration New, p.20 ↩
-
Original PDF page 21: L5 Wound healing and regeneration New, p.21 ↩
-
Original PDF page 22: L5 Wound healing and regeneration New, p.22 ↩
-
Original PDF page 23: L5 Wound healing and regeneration New, p.23 ↩
-
Original PDF page 24: L5 Wound healing and regeneration New, p.24 ↩
-
Original PDF page 25: L5 Wound healing and regeneration New, p.25 ↩
-
Original PDF page 26: L5 Wound healing and regeneration New, p.26 ↩
-
Original PDF page 27: L5 Wound healing and regeneration New, p.27 ↩
-
Original PDF page 28: L5 Wound healing and regeneration New, p.28 ↩
-
Original PDF page 29: L5 Wound healing and regeneration New, p.29 ↩
-
Original PDF page 30: L5 Wound healing and regeneration New, p.30 ↩
-
Original PDF page 31: L5 Wound healing and regeneration New, p.31 ↩
-
Original PDF page 32: L5 Wound healing and regeneration New, p.32 ↩
-
Original PDF page 33: L5 Wound healing and regeneration New, p.33 ↩
-
Original PDF page 34: L5 Wound healing and regeneration New, p.34 ↩
-
Original PDF page 35: L5 Wound healing and regeneration New, p.35 ↩
-
Original PDF page 36: L5 Wound healing and regeneration New, p.36 ↩
-
Original PDF page 37: L5 Wound healing and regeneration New, p.37 ↩
-
Original PDF page 38: L5 Wound healing and regeneration New, p.38 ↩
-
Original PDF page 39: L5 Wound healing and regeneration New, p.39 ↩
-
Original PDF page 40: L5 Wound healing and regeneration New, p.40 ↩
-
Original PDF page 41: L5 Wound healing and regeneration New, p.41 ↩
-
Original PDF page 42: L5 Wound healing and regeneration New, p.42 ↩
-
Original PDF page 43: L5 Wound healing and regeneration New, p.43 ↩
-
Original PDF page 44: L5 Wound healing and regeneration New, p.44 ↩
-
Original PDF page 45: L5 Wound healing and regeneration New, p.45 ↩
-
Original PDF page 46: L5 Wound healing and regeneration New, p.46 ↩
-
Original PDF page 48: L5 Wound healing and regeneration New, p.48 ↩
-
Original PDF page 47: L5 Wound healing and regeneration New, p.47 ↩