Conservative Pulp Treatment1
Some treatment dilemmas
Info
The primary dilemma for clinicians is deciding between performing a root canal treatment or attempting a more conservative pulp-preserving procedure. This decision is influenced by a variety of factors related to the tooth, the injury, and the patient’s restorative needs. The goal is to choose the treatment that offers the best long-term prognosis for the tooth.
- Pulp Exposures
- Trauma
- Caries
Pulp exposures from trauma2
Info
A pulp exposed due to a complicated crown or crown-root fracture is typically normal, healthy tissue. The management of such an exposure depends on several critical factors. its ability to respond to treatment is much greater than that of the pulp of a carious tooth
Main factors to consider in cases :
1. Diagnosis of pulp status
- depending on how long the patient waited until treatment, there may be some pulpitis
2. Stage of root development
Incompletely developed teeth3
AIM: Always wait for pulp revascularisation
- Allows further root development
- Improves long-term prognosis of tooth
Clinical Example
A study by Cvek (1992) demonstrated a direct correlation between the stage of root development and the frequency of root fractures, with the most immature teeth being the most vulnerable. A case was presented where premature root canal treatment on two very immature avulsed incisors resulted in a poor outcome. While one tooth was partially saved, the other had to be extracted due to a lack of further root development, highlighting the critical importance of attempting to preserve the pulp in such cases.
3. Other Concurrent injuries
Warning
The presence of other injuries, such as luxation, significantly impacts pulp survival. The more severe the concurrent injury (e.g., intrusion, lateral luxation), the lower the chance of pulp survival, especially in teeth with closed apices.
4 & 5 Size and time of exposure
Cvek Pulpotomy Study
Study by Cvek et al. found that partial pulpotomy is highly successful for traumatically exposed pulps, with success rates above 95%, regardless of exposure size or time.
Conclusion
This study strongly suggests that factors other than exposure size and time are more critical to healing, and that the partial pulpotomy is a highly predictable and successful procedure for traumatically exposed pulps.
6. Restorative Dental needs
Tip
For an immature tooth, a partial pulpectomy might be considered to allow for a post while preserving the apical pulp for further development.
Comprehensive list of factors for consideration45
- Diagnosis of pulp status
- Stage of root development
- Other concurrent injuries
- Size of exposure
- Time since exposure
- Restorative dental needs
Alternatives to endodontic treatment for pulp exposures6
Info
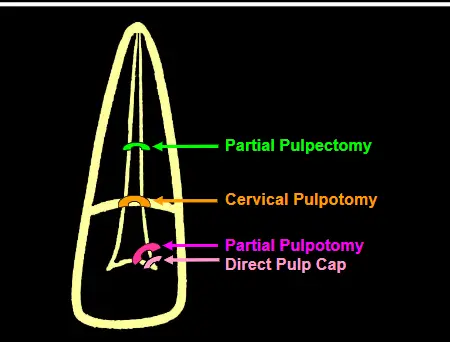
When root canal treatment is not indicated, several conservative options are available. These procedures are fundamentally similar, differing mainly in the level to which pulp tissue is removed.
Options:
- Pulp Capping
- Pulpotomy - Partial, Cervical - ==Partial Pulpotomy (Cvek Pulpotomy): Removal of the superficial 2–3 mm of inflamed/contaminated pulp tissue. - Full (Cervical) Pulpotomy: Removal of the entire coronal pulp down to the cervical level, typically used in anterior teeth with extensive fractures.==
- Pulpectomy - Partial
- Removal of pulp tissue to a deeper level within the root canal, often to accommodate a post while preserving the apical pulp in an immature tooth.
- Removal of pulp tissue to a deeper level within the root canal, often to accommodate a post while preserving the apical pulp in an immature tooth.
Aims of conservative treatment7
- Preserve the pulp
- Especially incompletely developed teeth
- Allow further root development
- Improves long-term prognosis
- “Stronger tooth”
- more dentine
- Improves long-term prognosis
Primary factor for consideration: pulp status8
- Diagnosis of pulp status must be
- Viable pulp
- Preferably no inflammation
- No necrosis or only surface necrosis at the site of exposure
Note
Conservative treatments are only viable for clinically normal pulps or those with reversible pulpitis. If the pulp has progressed to irreversible pulpitis or necrosis, root canal treatment is necessary.
Healing frequencies of conservative treatments8910
Exposed pulp after crown fractures
- Pulp Capping
- Placing a material directly onto a small pulp exposure. -72–81 %
- Partial Pulpotomy (Cvek) – 94–96 %
- Cervical Pulpotomy – 72–79 %
Partial pulpotomy healing rates compared with reported success rates for endodontic treatment they are fairly similar!:
Treatment of Choice
Given the exceptionally high success rate of the partial pulpotomy (94-96%), it is arguably the treatment of choice when clinically feasible.
Cvek partial pulpotomy technique11
- Used an abrasive high speed diamond bur with saline coolant
- Abrasive diamond - had no tissue damage beyond the wound surface
- ==Pulp Amputation: Use a high-speed diamond bur with copious water spray to create an abrasive wound. A diamond bur minimizes collateral tissue damage compared to a carbide bur, which tends to tear the pulp. The pulp is removed to a depth of approximately 2 mm.==
- ==Hemostasis (Bleeding Control): Place a cotton pellet moistened with sterile saline over the amputated pulp with gentle pressure for several minutes.==
- ==Assessment: If bleeding stops, it indicates that the remaining pulp tissue is healthy. If bleeding persists, the tissue is still inflamed, and a little more pulp must be removed until hemostasis is achieved.==
- ==Pulp Capping: Once bleeding is controlled, the chosen capping material is placed over the pulp stump.==
- ==Restoration: A base of glass ionomer is typically placed over the capping agent, followed by a final composite resin restoration.==
Note
It is not necessary to re-enter the tooth later to check for a dentine bridge. Success is determined by monitoring the tooth clinically (pulp sensibility tests) and radiographically (evidence of continued root development). A dentine bridge is a byproduct of healing, not a prerequisite for success, and re-entry causes unnecessary trauma.
Materials for pulp capping and pulpotomy1213
Choices:
- Calcium hydroxide
- Corticosteroid / Antibiotic
- Calcium Silicate-based Materials
Calcium hydroxide1314
-
Used for many years
-
Long history with good success rates
-
Considerable research
- Histological, clinical, radiographic, animals, humans, in vivo, in vitro, etc
-
Consistent findings & results
- ==A hard-setting formulation (e.g., Dycal, Life) must be used to provide a stable base for the final restoration.==
- The main limitation is the quality of the overlying restoration. If the seal fails, bacteria can colonize the necrotic zone created by the Ca(OH)₂ and lead to pulp infection.
Typical healing response with Ca(OH)₂15
(Cvek 1989)
- 1 = Necrosis
- 2 = Calcified tissue
- 3 = Dentine bridge
Corticosteroid/antibiotic combinations (Ledermix cement)15
Composition
- C-st: Triamcinolone - 0.67 %
- Ab: Demeclocycline - 2.0 %
- Calcium hydroxide - 33.4 %
- Zinc oxide - 47.2 %
- + Eugenol - 85% of the liquid
- Hard-setting base
Note
Essentially, it is a zinc oxide-eugenol (ZOE) cement fortified with calcium hydroxide, a corticosteroid, and an antibiotic.
Component properties16
Triamcinolone
-
Anti-inflammatory agent
- 70% released by the end of day 1
- Rest by end of day 3
-
NO evidence that it causes necrosis without symptoms
- Long held misconception about Ledermix cement
Debunking a Myth
The lecture strongly refutes the historical misconception that Ledermix causes asymptomatic pulp necrosis. This belief stemmed from its inappropriate use in the 1960s and 70s on teeth with irreversible pulpitis. The pulp was destined to necrose regardless; the drug merely masked the symptoms temporarily. When used correctly on vital, reversibly inflamed pulps, it is a safe and effective material.
Calcium hydroxide17
- Sedative and promotes dentine repair (numerous studies)
Zinc oxide - eugenol18
- The eugenol component is sedative and anti-inflammatory at low concentrations. The ZOE base also has antibacterial properties.
Release mechanism
- Eugenol is released by progressive hydrolysis
- Hydrolysis occurs at:
- External surface (saliva)
- Cavity floor (dentinal fluid)
Supporting evidence: Brännström’s studies192021
Brännström et al J Prosthet Dent 1979 Brännström’s “upside down restorations”
- Conclusion:
- ZO-E prevented entry of bacteria into the cavities
Typical healing response with Ledermix cement2223
- Normal pulp tissue in contact with the cement
- No inflammatory cells
- Occasionally a dentine bridge forms
- Occasionally diffuse calcifications in the pulp
Success
Healing often occurs with normal, non-inflamed pulp tissue directly in contact with the cement. A dentine bridge is seen less frequently than with calcium hydroxide, and its absence does not indicate failure. Clinical cases demonstrate excellent long-term pulp survival and continued root development in immature teeth treated with Ledermix cement.
Typical healing response - Ledermix cement (Robertson 1977)
Calcium silicate-based materials242526
- Examples:
- Mineral Trioxide Aggregate (MTA)
- Biodentine
ProRoot™ - mineral trioxide aggregate (MTA)27
Components
- Powder
- Dicalcium silicate
- Tricalcium silicate
- Tricalcium aluminate
- Bismuth oxide
- Calcium sulphate dihydrate
- Other trace elements
Note
MTA is primarily composed of dicalcium silicate, tricalcium silicate, and tricalcium aluminate, which are the main components of Portland cement.
- Liquid
- Sterile Water
Properties and performance28
Caution
While marketed as a all arounder, it doesn’t really repair internal resorption and a lot of its applications are very ituatinoal
Advantages
- Hard tissue formation; No inflammation
- Excellent mechanical properties
- But studies have not shown any advantage over Ca(OH)₂
Disadvantages
- Difficult to handle the material
- Powder + sterile water - ratio critical
- It is difficult to handle, with a consistency similar to wet sand or concrete.
- Powder + sterile water - ratio critical
- Very slow setting time - at least 4 hours
- This complicates the placement of an immediate final restoration.
- Discolouration of the tooth
- Especially with the original grey version
- But also with the later white version
-
This is a significant aesthetic concern for anterior teeth.
-
Although less severe
-
Biodentine29
Components
- Powder
- Tricalcium silicate
- Calcium carbonate
- Zirconium oxide
- Liquid
- Calcium chloride
- Accelerator
- Water
- Calcium chloride
Advantages30
- Easier to mix and handle than MTA
- Capsule
- Faster setting time than MTA
- 10-12 minutes
- Does not discolour the tooth
- Recommended as a “dentine replacement” material
- Can be used as a coronal restorative material
- Excellent mechanical properties
- Pulp cap: excellent pulp responses and dentine bridges
Footnotes
-
Original PDF page 1: O10A Conservative Pulp Treatment, p.1 ↩
-
Original PDF page 2: O10A Conservative Pulp Treatment, p.2 ↩
-
Original PDF page 3: O10A Conservative Pulp Treatment, p.3 ↩
-
Original PDF page 8: O10A Conservative Pulp Treatment, p.8 ↩
-
Original PDF page 9: O10A Conservative Pulp Treatment, p.9 ↩
-
Original PDF page 10: O10A Conservative Pulp Treatment, p.10 ↩
-
Original PDF page 11: O10A Conservative Pulp Treatment, p.11 ↩
-
Original PDF page 12: O10A Conservative Pulp Treatment, p.12 ↩ ↩2
-
Original PDF page 13: O10A Conservative Pulp Treatment, p.13 ↩
-
Original PDF page 14: O10A Conservative Pulp Treatment, p.14 ↩
-
Original PDF page 15: O10A Conservative Pulp Treatment, p.15 ↩
-
Original PDF page 16: O10A Conservative Pulp Treatment, p.16 ↩
-
Original PDF page 17: O10A Conservative Pulp Treatment, p.17 ↩ ↩2
-
Original PDF page 18: O10A Conservative Pulp Treatment, p.18 ↩
-
Original PDF page 19: O10A Conservative Pulp Treatment, p.19 ↩ ↩2
-
Original PDF page 20: O10A Conservative Pulp Treatment, p.20 ↩
-
Original PDF page 21: O10A Conservative Pulp Treatment, p.21 ↩
-
Original PDF page 22: O10A Conservative Pulp Treatment, p.22 ↩
-
Original PDF page 23: O10A Conservative Pulp Treatment, p.23 ↩
-
Original PDF page 24: O10A Conservative Pulp Treatment, p.24 ↩
-
Original PDF page 25: O10A Conservative Pulp Treatment, p.25 ↩
-
Original PDF page 26: O10A Conservative Pulp Treatment, p.26 ↩
-
Original PDF page 27: O10A Conservative Pulp Treatment, p.27 ↩
-
Original PDF page 28: O10A Conservative Pulp Treatment, p.28 ↩
-
Original PDF page 29: O10A Conservative Pulp Treatment, p.29 ↩
-
Original PDF page 30: O10A Conservative Pulp Treatment, p.30 ↩
-
Original PDF page 31: O10A Conservative Pulp Treatment, p.31 ↩
-
Original PDF page 32: O10A Conservative Pulp Treatment, p.32 ↩
-
Original PDF page 33: O10A Conservative Pulp Treatment, p.33 ↩
-
Original PDF page 34: O10A Conservative Pulp Treatment, p.34 ↩