Occlusion and mandibular movements1
Mandibular movements2
Description of movements depends on the viewer perspective or viewer’s position.
Note
To fully describe the complex, three-dimensional movement of the mandible, it must be broken down and analyzed from three distinct planes.
Planes of movement34
Info
A single movement of the jaw will have a different trajectory when projected onto each of the three anatomical planes. To completely describe a mandibular movement, one must specify the plane of observation.
Mandibular border movements5678910
- Maximum extension of the mandibular motion
- Reference points
Tip
In contrast, functional movements, such as chewing and speaking, occur within the boundaries established by these border movements.
Overview of movements by plane
-
Sagittal plane:
- Protrusion and opening
- Lateral movements are not clearly visible as the object only appears to change size.
-
Horizontal plane:
- Laterotrusion
- Opening is not visible.
-
Frontal plane:
- Lateral and opening
- Protrusion is not visible.
Border movements in detail12
Sagittal plane
Note
The starting point for describing sagittal plane movements is Centric Relation (CR), a slightly retruded position where the condyles are in their optimal position within the glenoid fossa, and there is no tooth contact.
Centric relation: a maxillomandibular relationship independent of tooth contact, the condyles articulate in the anterior-superior position against the posterior slopes of the articular eminences.
Superior contact border movements13141516171819
This path is traced when the teeth are in contact.
- CR to MIP: The jaw moves slightly up and forward from centric relation to the maximum intercuspal position (MIP), also known as the intercuspal position (ICP).
- Anterior guidance: From MIP, as the mandible protrudes, the lower incisors glide along the lingual surfaces of the upper incisors, causing posterior disocclusion.
- Edge-to-edge: The protrusive movement continues until the incisors meet edge-to-edge, which appears as a plateau on the movement diagram.
- Maximum protrusion: Moving past the edge-to-edge position, the jaw can close slightly more as it reaches its maximum forward limit.
Posterior opening border movements2021
-
1st stage:
- Pure rotation of condyle
- Terminal hinge axis
- Up to 2 cm of opening
-
2nd stage:
- Rotation + translation
- As opening continues towards the maximum, the condyles translate forward and downward. This changes the arc of the opening path.
- Rotation + translation
-
Maximum opening
Anterior opening border movements22
Info
This path connects the anterior and posterior limits of movement. From the maximum opening position, the jaw closes while moving forward, tracing a path up to the point of maximum protrusion.
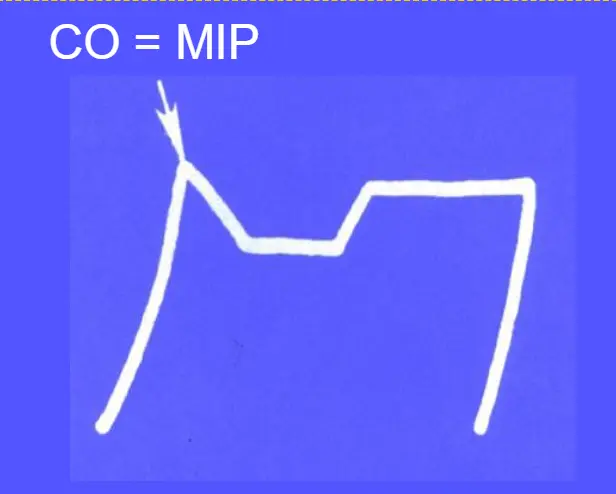
Summary of sagittal plane movements2324
- Posterior opening border
- Anterior opening border
- Superior contact border
- Typical functional movements – chewing (not part of the border movements)

Note
If a patient’s centric occlusion (CO), which is the occlusion in centric relation, coincides with their MIP, the starting point of the superior contact path will be the same as the endpoint of the initial closure.
Effect of head position25

Head posture significantly affects mandibular position and must be controlled during clinical procedures like bite registration.
- ==Upright Position: This is the ideal position for capturing a patient’s true MIP. The patient should be sitting upright without a headrest.==
- ==Head Tilted Backwards: The depressor muscles of the mandible are stretched, causing the jaw to retrude. A bite registration taken in this position may inadvertently capture CR or a position between CR and MIP.==
- ==Head Tilted Forwards: Gravity will pull the mandible forward, leading to an inaccurate, protruded bite registration.==
Clinical Relevance
This is especially critical for fabricating full dentures, where there are no existing teeth to guide the patient into MIP. An incorrect bite registration due to head posture can lead to a prosthesis with a poor fit and function. Final occlusal adjustments on any restoration should be double-checked with the patient sitting upright.
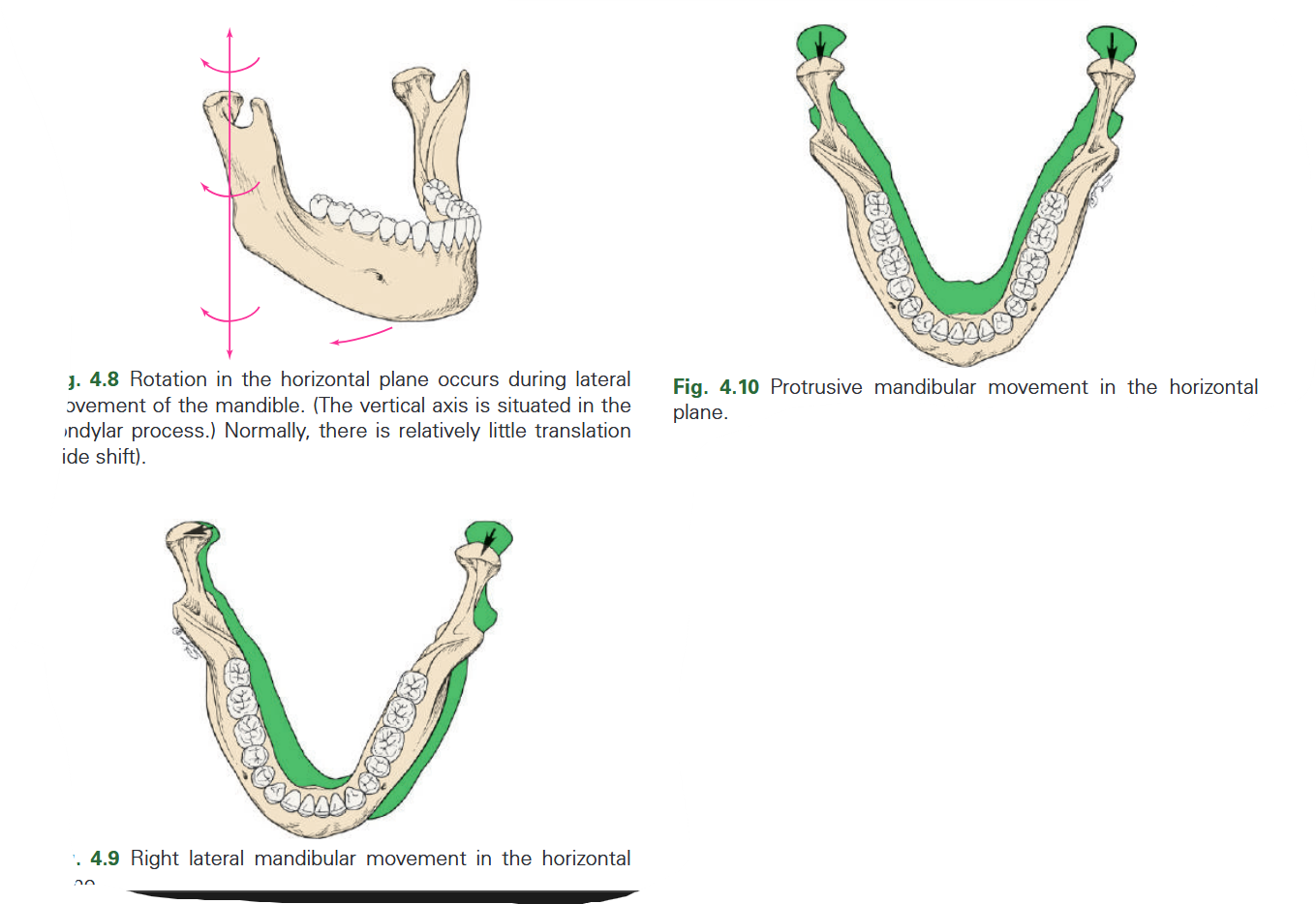
Horizontal plane2627
Info
Movements in this plane are viewed from above, tracing a diamond or shield shape. The starting point is centric relation (CR).
Maximum laterotrusion left
Note
From the left lateral position, it moves in a forward arc to maximum protrusion. During this phase, both lateral pterygoid muscles are contracting.
Note
From the right lateral position, it moves in another forward arc back to maximum protrusion, completing the envelope.
Summary of horizontal plane movements28293031
- Lateral to the left
- Lateral to the left followed by protrusion
- Lateral to the right
- Lateral to the right followed by protrusion

Tip
MIP is typically located slightly anterior to CR.
Functional movements in the horizontal plane32
Info
The pattern of chewing movements (masticatory cycle) varies with the food being chewed.
Tip
The edge-to-edge position is outside the normal functional chewing cycle for a person with a normal occlusion.
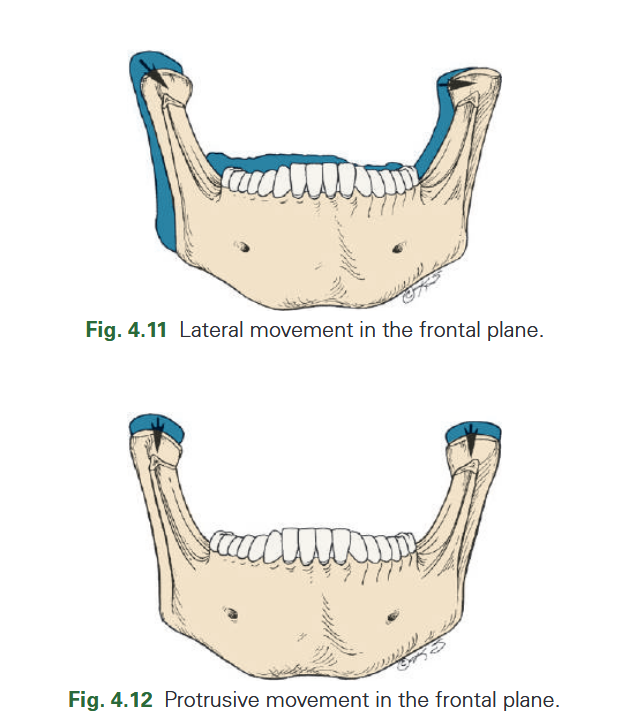
Frontal plane33
Info
Movements in this plane are viewed from the front, starting from MIP.
- From MIP, the jaw moves laterally. The path is typically concave (curving upwards) due to guidance from the canines (canine guidance) or posterior teeth (group function).
- From the maximum lateral position, the jaw opens to the point of maximum opening.
- The jaw then closes back towards MIP, often moving to the opposite side to begin the next cycle. The paths are often not symmetrical.
Summary of frontal plane movements34353637
-
Superior lateral to the right
-
Opening lateral to the right
-
Superior lateral to the left
-
Opening lateral to the left
-
PP = Postural position
-
Postural position (PP) is the relaxed state of the mandible, with the masticatory muscles in a state of tonic contraction and no tooth contact. It is located slightly below MIP and corresponds to the rest vertical dimension.
-
Functional (chewing) cycle: This is a smaller teardrop-shaped loop within the border envelope.
- In a patient with good canine guidance, the chewing cycle typically starts and ends at the same point (MIP).
- In a patient with worn dentition and no canine guidance, the start and end points of the cycle are less consistent.
Posselt’s envelope of mandibular movement3839
Abstract
When the border movements from all three planes (sagittal, horizontal, and frontal) are combined, they form a three-dimensional solid figure known as Posselt’s envelope of motion. This envelope represents the total space within which the mandible can move. The surfaces of the envelope are determined by the anatomy of the TMJs, ligaments, and teeth.
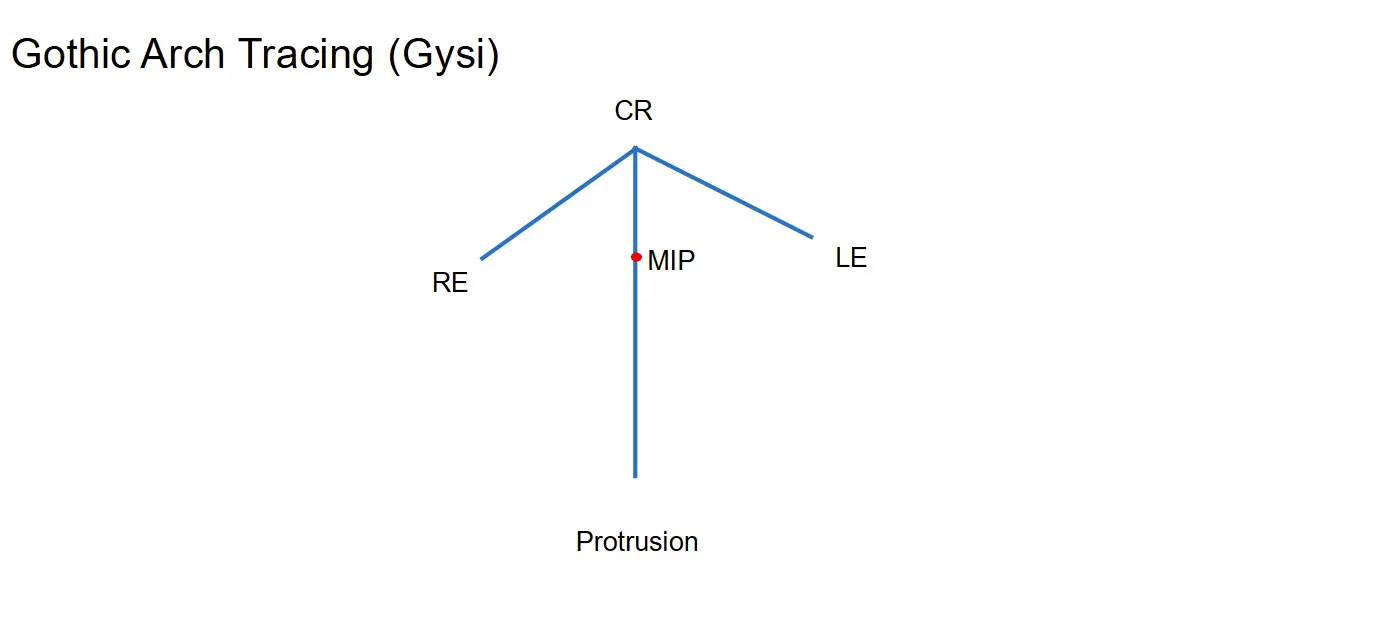
Gothic arch tracing (Gysi)40
Info
A Gothic arch tracing is a simplified, two-dimensional recording of the horizontal border movements, often used in the fabrication of full dentures.
- Mechanism: A pin attached to one dental arch traces movements onto a platform attached to the opposing arch.
- Interpretation: The tracing creates an arrowhead shape. The sharp tip of the arrow represents centric relation (CR), and the two sides represent the paths of left and right lateral movements.
- Clinical use: It helps clinicians verify the CR position and see its relationship to MIP. It can identify a long centric (MIP is anterior to CR) or an eccentric position (MIP is to the side of the path from CR).
Pantograph414243
- Pantographic tracing
Note
These recordings can then be used to program a fully adjustable articulator to replicate the patient’s unique jaw movements.
Digital pantograph44
- Designed to record and measure functional and border movements
- Possible to adjust digital articulators automatically
Research applications
Modern digital pantographs are used in research to study and assess masticatory function. Studies show that chewing patterns vary and provide diagnostic information:
- Soft food: Many cycles, narrow width.
- Hard food: Fewer cycles, wider opening.
- Chewing gum: Fewer cycles, very wide movements.
- Canine guidance: A consistent, repeatable chewing cycle that starts and ends at MIP.
- Worn dentition: A less consistent cycle without a single, defined start/end point.
- Malocclusion/disc displacement: An arbitrary, non-patterned movement, indicating dysfunction.
Frontal plane
Biomechanics of mandibular movements454647
The mandible as a lever system48495051
The mandible is a Class III Lever
Info
- Fulcrum: The condyle within the TMJ.
- Effort: The contraction of the masticatory muscles (e.g., masseter, temporalis).
- Load: The food bolus being crushed between the teeth.
Biomechanical advantage
Although mechanically inefficient, the class III lever design is highly advantageous for the jaw because it preserves and protects the fulcrum (the TMJ) from excessive forces. If the muscle insertion were further from the joint (like a class II lever), the forces on the condyle and disc would be immense. This system also protects the teeth. The greatest biting force is generated closest to the muscle attachment (effort), which is in the molar region. The molars are structurally designed to withstand these high forces. The anterior teeth, being further from the muscle, receive significantly less pressure, which is consistent with their function of incising and guiding, not heavy grinding. This highlights the importance of creating restorations that function in harmony with the existing biomechanical system.
Footnotes
-
Original PDF page 1: M5 Mandibular Movments, p.1 ↩
-
Original PDF page 3: M5 Mandibular Movments, p.3 ↩
-
Original PDF page 4: M5 Mandibular Movments, p.4 ↩
-
Original PDF page 5: M5 Mandibular Movments, p.5 ↩
-
Original PDF page 6: M5 Mandibular Movments, p.6 ↩
-
Original PDF page 7: M5 Mandibular Movments, p.7 ↩
-
Original PDF page 8: M5 Mandibular Movments, p.8 ↩
-
Original PDF page 9: M5 Mandibular Movments, p.9 ↩
-
Original PDF page 10: M5 Mandibular Movments, p.10 ↩
-
Original PDF page 11: M5 Mandibular Movments, p.11 ↩
-
Original PDF page 12: M5 Mandibular Movments, p.12 ↩
-
Original PDF page 13: M5 Mandibular Movments, p.13 ↩
-
Original PDF page 14: M5 Mandibular Movments, p.14 ↩
-
Original PDF page 15: M5 Mandibular Movments, p.15 ↩
-
Original PDF page 16: M5 Mandibular Movments, p.16 ↩
-
Original PDF page 17: M5 Mandibular Movments, p.17 ↩
-
Original PDF page 18: M5 Mandibular Movments, p.18 ↩
-
Original PDF page 19: M5 Mandibular Movments, p.19 ↩
-
Original PDF page 20: M5 Mandibular Movments, p.20 ↩
-
Original PDF page 21: M5 Mandibular Movments, p.21 ↩
-
Original PDF page 22: M5 Mandibular Movments, p.22 ↩
-
Original PDF page 23: M5 Mandibular Movments, p.23 ↩
-
Original PDF page 24: M5 Mandibular Movments, p.24 ↩
-
Original PDF page 25: M5 Mandibular Movments, p.25 ↩
-
Original PDF page 26: M5 Mandibular Movments, p.26 ↩
-
Original PDF page 27: M5 Mandibular Movments, p.27 ↩
-
Original PDF page 28: M5 Mandibular Movments, p.28 ↩
-
Original PDF page 29: M5 Mandibular Movments, p.29 ↩
-
Original PDF page 30: M5 Mandibular Movments, p.30 ↩
-
Original PDF page 31: M5 Mandibular Movments, p.31 ↩
-
Original PDF page 32: M5 Mandibular Movments, p.32 ↩
-
Original PDF page 33: M5 Mandibular Movments, p.33 ↩
-
Original PDF page 34: M5 Mandibular Movments, p.34 ↩
-
Original PDF page 35: M5 Mandibular Movments, p.35 ↩
-
Original PDF page 36: M5 Mandibular Movments, p.36 ↩
-
Original PDF page 37: M5 Mandibular Movments, p.37 ↩
-
Original PDF page 38: M5 Mandibular Movments, p.38 ↩
-
Original PDF page 39: M5 Mandibular Movments, p.39 ↩
-
Original PDF page 40: M5 Mandibular Movments, p.40 ↩
-
Original PDF page 41: M5 Mandibular Movments, p.41 ↩
-
Original PDF page 42: M5 Mandibular Movments, p.42 ↩
-
Original PDF page 43: M5 Mandibular Movments, p.43 ↩
-
Original PDF page 44: M5 Mandibular Movments, p.44 ↩
-
Original PDF page 45: M5 Mandibular Movments, p.45 ↩
-
Original PDF page 46: M5 Mandibular Movments, p.46 ↩
-
Original PDF page 47: M5 Mandibular Movments, p.47 ↩
-
Original PDF page 48: M5 Mandibular Movments, p.48 ↩
-
Original PDF page 50: M5 Mandibular Movments, p.50 ↩
-
Original PDF page 51: M5 Mandibular Movments, p.51 ↩
-
Original PDF page 52: M5 Mandibular Movments, p.52 ↩
-
Original PDF page 53: M5 Mandibular Movments, p.53 ↩