- Major infections of Mouth and face July 18, 2025 9:18 AM
Bacterial infections
Bacterial infections are caused by microorganisms. The lecture covers three key bacterial infections relevant to the oral and maxillofacial region.
Oral Actinomycosis
- Actinomycosis is a chronic, suppurative infection caused by Actinomyces sp . Although common in the past, it has become rare.
- Half of all cases affect the face and neck.
- Clinically, men are predominantly affected, ages 30 and 60 years.
- Chronic soft tissue swelling near the angle of the jaw in the upper neck is the usual complaint.
- Pain is minimal.
- The usual clinical features are a persistent subcutaneous collection of pus or a sinus, unresponsive to conventional, short courses of antibiotics.
- A bacterial culture is required to identify the organism, and treatment involves a specific, long-term antibiotic regimen.
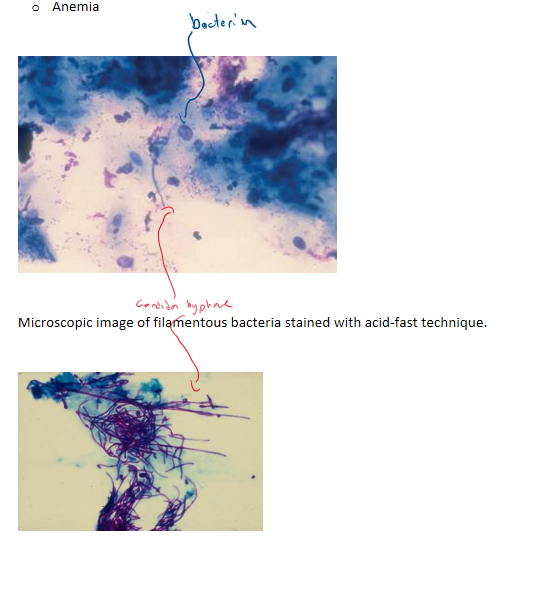
- Actinomyces israelii is a long filamentous Gram-positive bacterium, not a fungus as its name suggests.
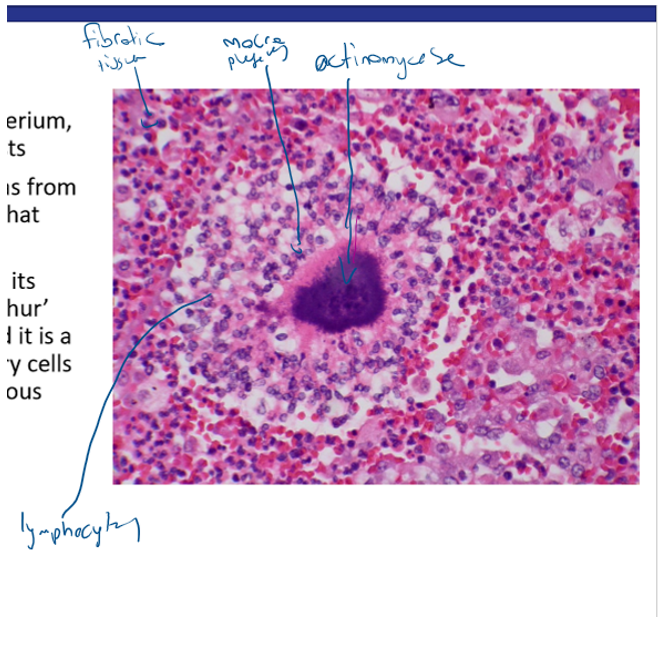
- This single, complete loculus was from an early case of actinomycosis that followed dental extraction.
- The colony of actinomyces with its paler staining periphery (a ‘sulphur’ granule) is in the centre; around it is a dense collection of inflammatory cells surrounded by proliferating fibrous tissue. Microscopically, the bacterial colonies show a central basophilic mass. These are surrounded by a dense infiltrate of chronic inflammatory cells, along with collections of neutrophils, consistent with suppuration.
Tuberculosis
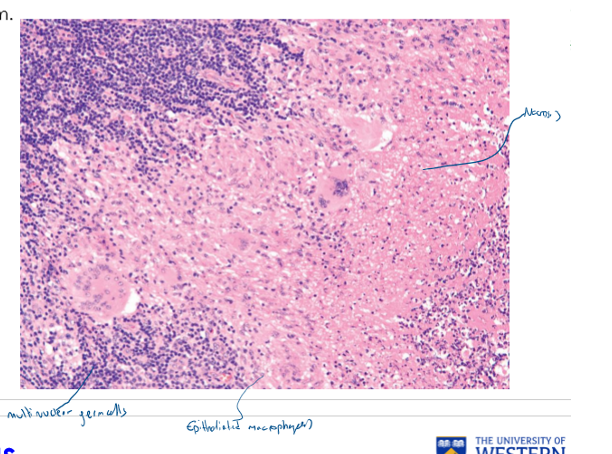
Tuberculosis is the second most common cause of death from a single infectious agent worldwide, after HIV/AIDS. The incidence is increasing, partly due to its association with the rising number of HIV-positive patients. It is more common in individuals with low socioeconomic status, poor nutrition, or severe systemic conditions that compromise the immune system. Oral lesions are noted in less than 5% of patients with pulmonary tuberculosis. Occurs in the second to fourth decades of life and presents as an ulcer of the oral mucosa, a mass or osteolytic lesions within the jawbones, with some patients exhibiting tuberculous lymphadenitis (scrofula) and salivary gland involvement. Mycobacterium tuberculosis, a facultative intracellular bacterium. Histopathologically, tuberculosis is characterized by granulomatous inflammation, featuring a central area of caseous necrosis, multinucleated giant cells, and large epithelioid macrophages. The bacteria can be identified using a special stain called the Ziehl-Neelsen stain.
Tip
A key tel lof Tb is the necrotic areas, if there is no necrosis then it will probably be some other condition Zeihl-nielson stains for this bacteria
SYPHILIS
Syphilis is a chronic bacterial disease that is endemic in low- and middle- income countries, and those in economically depressed neighborhoods. More than 5 million new cases of syphilis are diagnosed every year. If left untreated, it can lead to irreversible neurological and cardiovascular complications. 91% of all cases occur in men, and it is closely linked with HIV infection.
Types
- Primary syphilis (chancre)
- Secondary syphilis
- Tertiary syphilis
- Congenital syphilis
Pathobiology
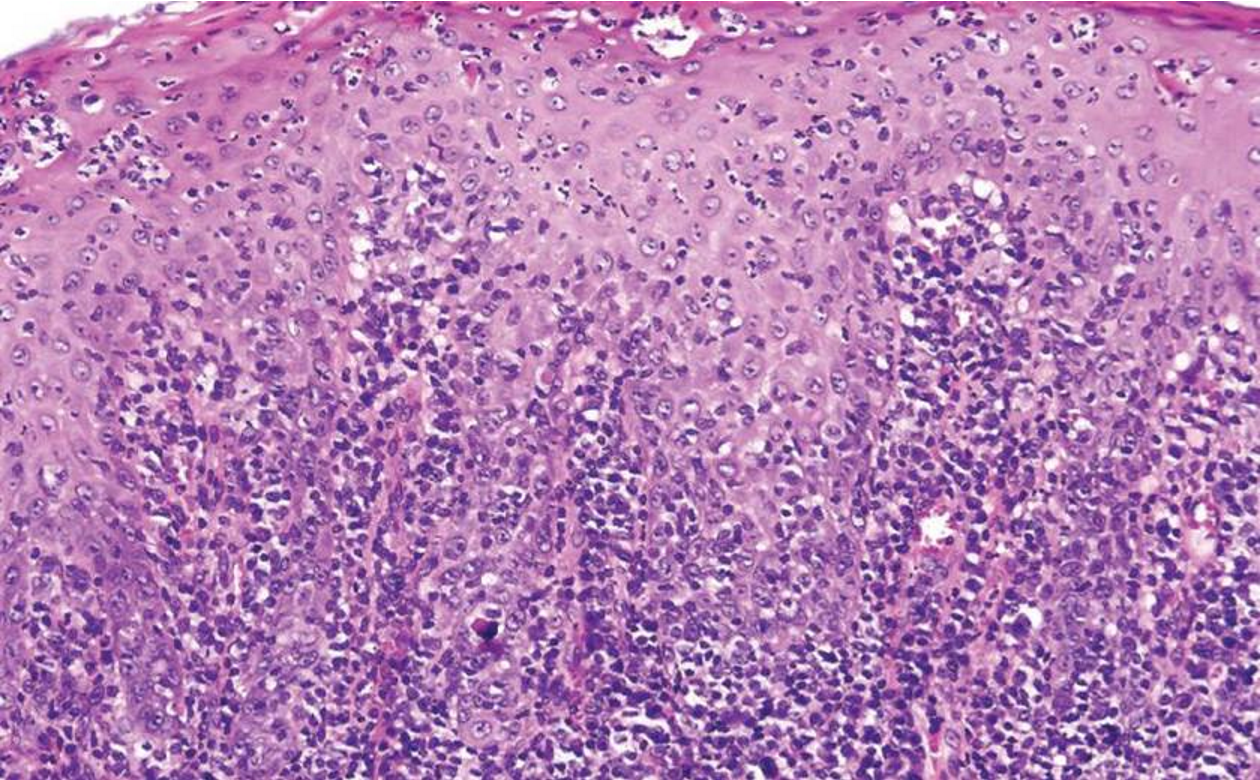
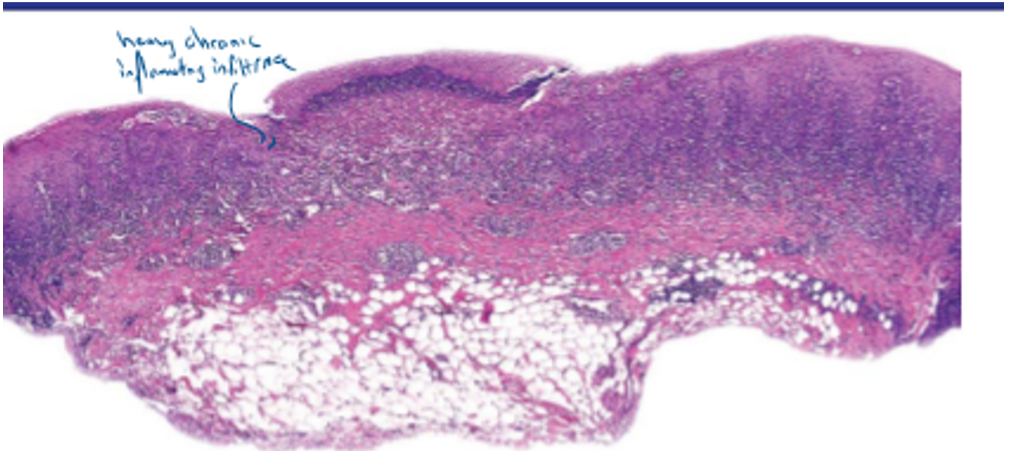
The spirochete responsible for this disease is Treponema pallidum . The infection triggers a dense lymphocytic infiltrate that gathers around blood vessels deep within the connective tissue and can affect the entire epithelium. Confirmation of the diagnosis often requires a qPCR test to detect the microorganism’s DNA. Syphillis appears as an ulcer
- For syphillis and tuberculosis its recommended to do PCR to confirm the prescence of the pathogen
Viral Infections
Herpesviruses
Herpesviruses are DNA viruses that are mostly:
- transmitted in saliva.
- characterised by latency.
- Latency is typically established in the sensory nerve ganglia of facial nerves.
- reactivated during immunosuppression.
- cause more severe disorders in patients with compromised immunity, HIV, cancer patients and those immunosuppressed after organ grafts.
Herpesvirus Types
| Herpesvirus Type | Disease Manifestation |
|---|---|
| HHV-1 | Oral cavity: Primary herpetic gingivostomatitis and recrudescent herpes stomatitis or herpes labialis |
| Herpes simplex virus-1 | Genital herpes, eczema herpeticum, herpes whitlow, herpes gladiatorum, ocular herpes, herpes encephalitis, disseminated infection |
| Alpha virus | |
| HHV-2 | Although usually found on skin and mucosa below the waist (genital herpes), may also be found in the mouth with lesions identical to those of HSV-1, neonatal infection, herpetic whitlow (also see HHV-1 above) |
| Herpes simplex virus-2 | |
| Alpha virus | |
| HHV-3 | Oral cavity: Primary infection exhibits oral ulcers; recrudescent infection is facial or oral shingles along the distribution of the trigeminal nerve and is usually unilateral |
| Varicella-zoster virus | Primary infection is chickenpox; skin shingles are common on the trunk |
| Alpha virus | |
| HHV-4 | Oral cavity: Hairy leukoplakia occurs in patients with HIV/AIDS, organ transplant recipients, or other immunocompromised hosts, as well as those on immunosuppressive agents; not infrequently occurs in the healthy host |
| Epstein-Barr virus | Epstein-Barr virus mucocutaneous ulcer in immunosuppressed or immunosenescent host Infectious mononucleosis, Burkitt lymphoma, central nervous system lymphoma, diffuse large B-cell lymphoma, NKT lymphoma, immunodeficiency-associated lymphoproliferative disorder, Hodgkin lymphoma, plasmablastic lymphoma, nasopharyngeal carcinoma, leiomyosarcoma, follicular dendritic cell sarcoma |
| Gamma virus | |
| HHV-5 | Oral cavity: Penetrating oral ulcers; organism may be a bystander noted in other ulcerative lesions |
| Cytomegalovirus | Infectious mononucleosis-like syndrome, retinitis, gastroenteritis, hepatitis, pneumonitis |
| Beta virus | |
| HHV-6 | No documented oral findings |
| Beta virus | Roseola infantum, exanthema subitum |
| HHV-7 | No documented oral findings |
| Beta virus | Roseola infantum, exanthema subitum |
| HHV-8 | Oral cavity: Kaposi sarcoma |
| Kaposi sarcoma herpesvirus | Skin and visceral Kaposi sarcoma, primary effusion lymphoma, multicentric Castleman disease, diffuse large B-cell lymphoma |
| Gamma virus |
Herpes simplex virus
The primary clinical infection with HSV:
- Usually caused by HSV-1
- Seen mainly between the ages of 2 and 4 years.
- Increasingly seen in older patients.
- In teenagers, sometimes due to HSV-2 transmitted sexually and mainly cause oropharyngeal soreness.
Predisposing factors
- Herpes simplex virus is contracted from infected saliva or other body fluids after 4-7 days of incubation
- Close contact with infected individuals
- HSV-1 can cause oral and oropharyngeal infection (above belt)
- HSV-2 is traditionally associated with genital infections, but this distinction is becoming less clear due to practices like oral sex.
- HSV-2 can cause severe oropharyngeal infection usually via orogenital or oro-anal sexual contact.
- Patients with immune defects are liable to infections.
Primary herpetic gingivostomatitis
- common herpesvirus infection in the first three decades of life
- fever, malaise, and sore throat, followed by an acute onset of multiple, painful, clustered, and subsequently coalescent ulcers on any mucosal surface, but frequently on the lip mucosa, tongue, and gingiva
- The ulcers can spread and even aggregate with each other
- Before rupture of the blister, the patient is still infectious
Herpes labialis
- Herpes labialis on the lip (fever blisters or cold sores) is the most common presentation with less common sites being the keratinized mucosa of the hard palatal mucosa and attached gingiva.
- The infection starts as painful, clustered vesicles (blisters) which then rupture, leaving ulcers covered by a fibrinous exudate that eventually crusts over.
- There are painful, 2- to 3-mm clustered and coalescent ulcers with scalloped borders often induced by injury (e.g., sunburn) or trauma (e.g., dental procedures).
Primary varicella-zoster virus
- This infection causes vesicles on erythematous skin and also in the mouth that rupture to form ulcers.
- Reactivation of VZV tends to occur in older adults, in immunocompromised hosts, and in those on biological therapies such as tumor necrosis factor inhibitors.
Pathobiology
- HSV and VZV are DNA viruses that are cytotoxic to epithelial cells.
- The virus enters epithelial cells, replicates, and causes the cells to rupture, releasing new viral particles to infect adjacent cells. This cellular destruction leads to the formation of fluid-filled blisters, which then rupture to leave behind painful ulcers. Lesions typically heal within 7-10 days, even without treatment. After primary infection, latency is established in sensory ganglia and peripherally at mucosal sites. Reactivation of HSV either leads to asymptomatic shedding, which is the primary means of transmission, or results in painful lesions, referred to as recrudescence.
HAIRY LEUKOPLAKIA
- caused by the Epstein-Barr virus (EBV)
- It is considered a leading clinical sign of HIV infection.
- occurs most commonly in immunocompromised individuals, especially those with HIV/ AIDS with low CD4 counts and in organ transplant recipients.
- Healthy patients, usually older adults, possibly due to immunosenescence
- Clinically appears a white, painless, linear lesion or plaque, usually on the lateral border of tongue, and cases are usually bilateral. Classically, white linear lesions run perpendicular to the long axis of the tongue. The white lesion is non-removable.
Pathobiology
- EBV establishes latency in peripheral memory B lymphocytes and one theory proposes that these B lymphocytes migrate to the lamina propria or to the oral epithelium where EBV undergoes productive replication resulting in hairy leukoplakia.
- Histologically, there is a significant thickening of the stratified squamous epithelium. A key feature is the presence of viral inclusion bodies within the epithelial cells, and a definitive diagnosis requires special staining to confirm the presence of EBV.
HUMAN PAPILLOMAVIRUS—RELATED BENIGN LESIONS
- Squamous papilloma, verruca vulgaris, condyloma acuminatum and Heck disease (focal epithelial hyperplasia)
- The lesion has a verrucous appearance with a very corrugated, thick keratin surface. It is characterized by blunt, broad, and bulky rete ridges., condyloma acuminatum, and Heck disease (focal epithelial hyperplasia
- These lesions are caused by Human Papillomavirus (HPV), a large family of over 100 virus types. HPV types are broadly classified as low-risk, which cause benign lesions, and high-risk, which are associated with malignant tumors. The following lesions are caused by low-risk HPV types.)
- Young patients present as painless, exophytic, papillary/verrucous or papular, white or pink, sessile, or pedunculated growths on the mucosa.
Squamous papilloma
- This is often seen on the soft palate and hard palatal mucosa, tongue or gingiva and may be white/keratotic or mucosal-colored, and is only a few millimeters in size.
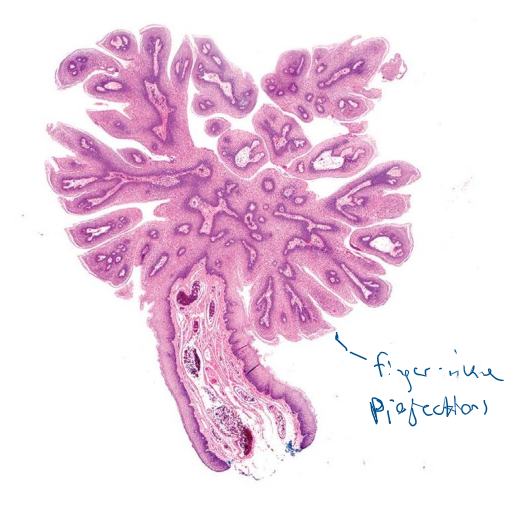

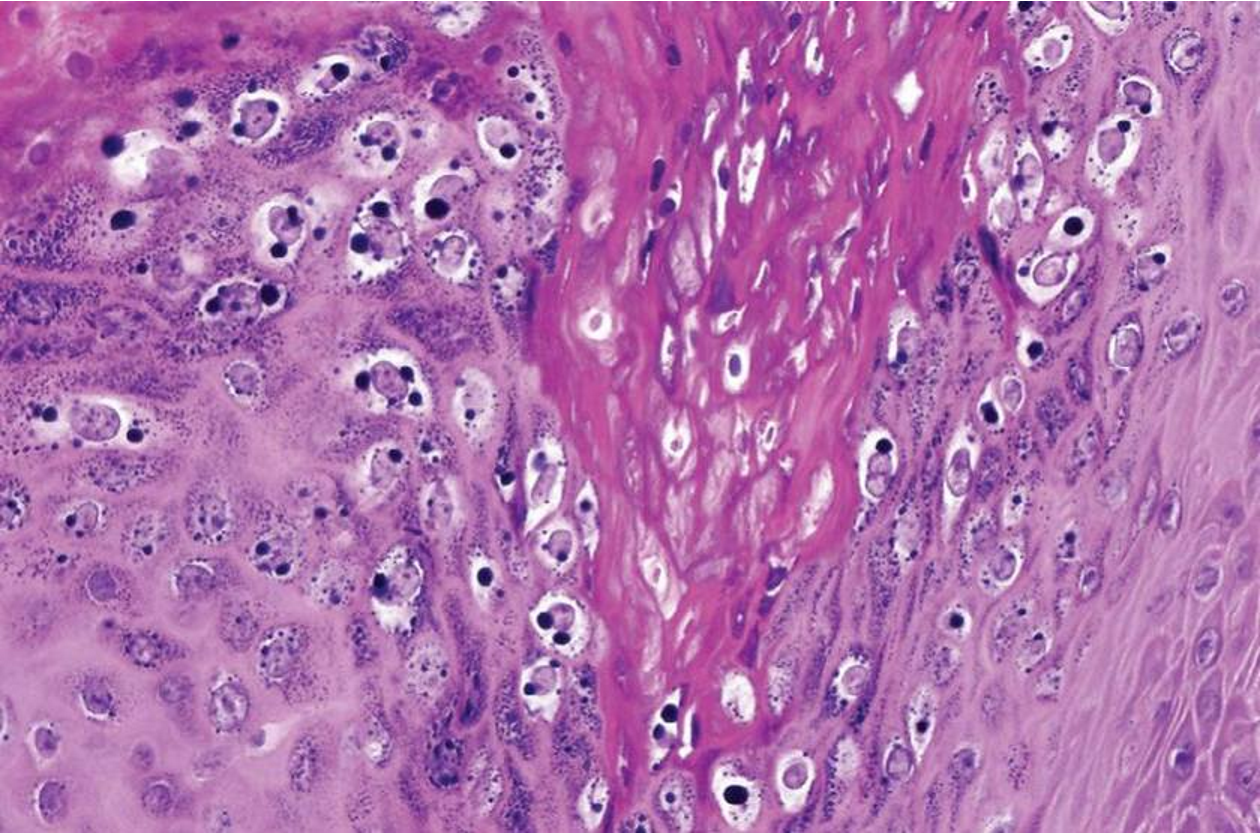
- black arrows are cells infected by hpv
Histopathology
Squamous papilloma
- Caused by HBV type 6 and 8
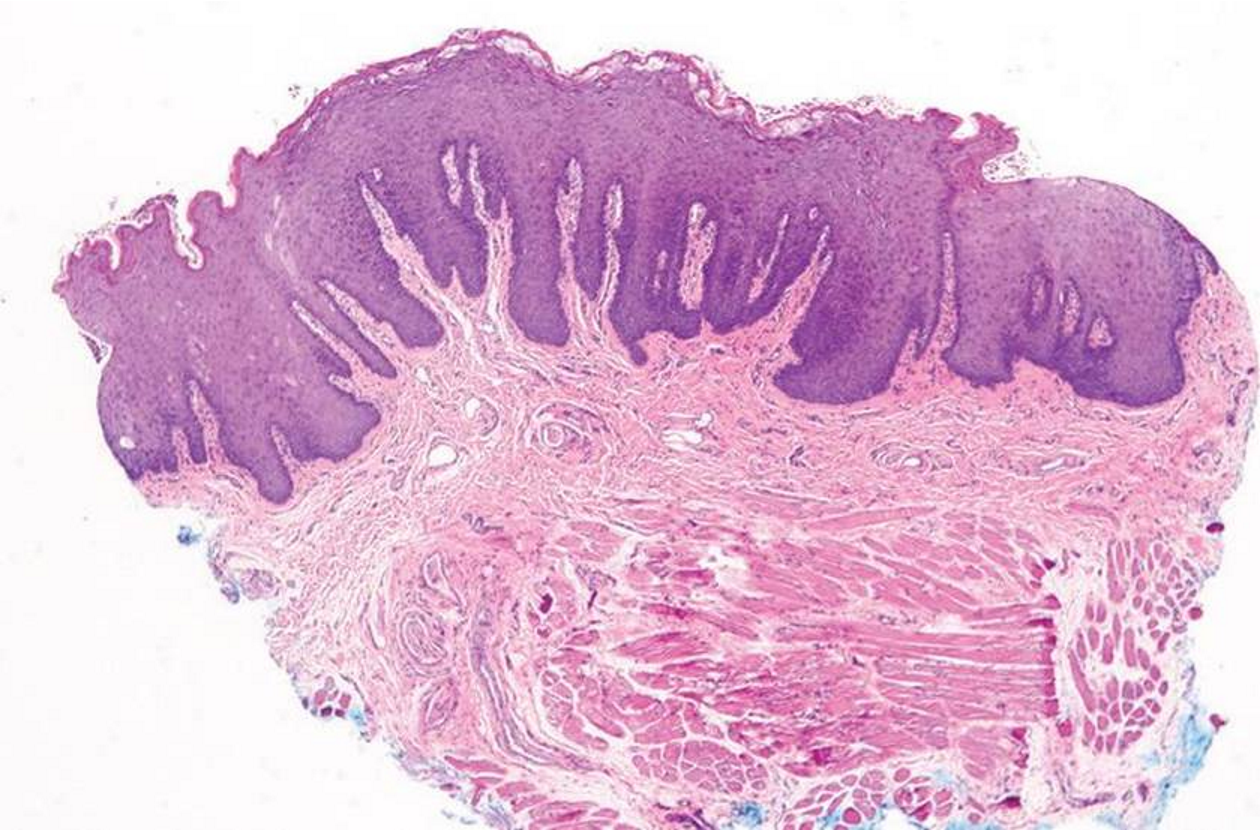
Verruca vulgaris
- This is often on the gingiva, lips, and palatal mucosa and is almost always white/keratotic, and is only a few millimeters in size.
- Clinically appears as a verccous lesion that is small (only a few mm in diameter)

Histopathology

Condyloma acuminatum

- This is usually seen in immunocompromised patients as single or multiple papular or papillary lesions that are mucosal-colored and usually 1 cm in size or larger.
- Their presence can also be associated with poor oral hygiene.
Histopathology
Condyloma acuminatum The lesion shows broad, elongated rete ridges and acanthosis (thickening of the epithelium). Viral inclusions are present in the epithelial cells, which can be confirmed with a special stain for HPV.
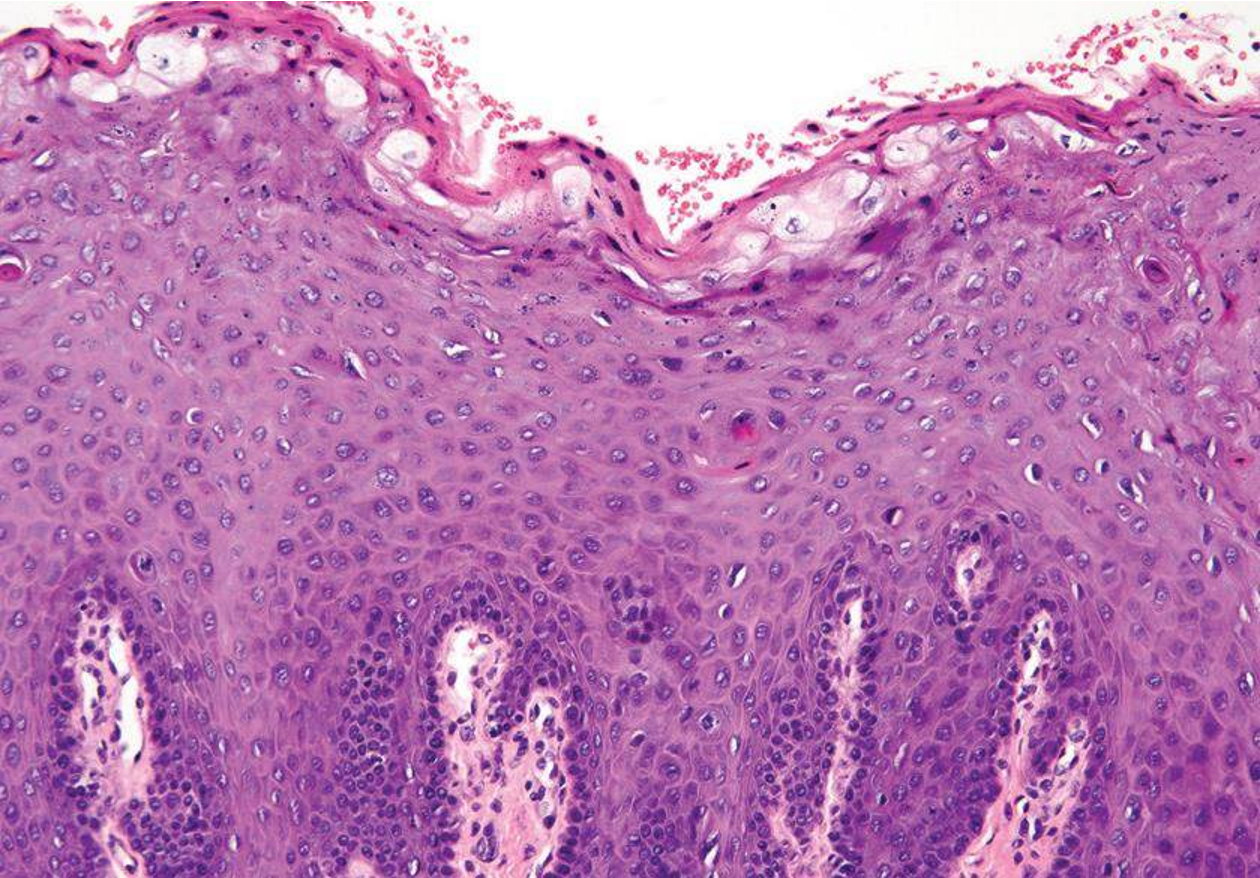
Heck disease

There are multiple papules/nodules or papillary lesions (less common), several millimeters in size, but may coalesce to form larger lesions on the mucosa of the lips and tongue, often seen in the first and second decades of life. It occurs in up to 13% of those living in crowded South and Central America conditions. It is also common in Africa, the Middle East, in patients with HIV/AIDS, and sporadically in North America. The condition tends to regress with age when lesions begin in childhood.
- Most likely there is a family history as well especially with heck disease
Histopathology
- The lesion features thickened stratified squamous epithelium with a thickened keratin layer.
- The rete ridges are elongated and have an irregular shape.
- The superficial epithelial cells have a characteristic
Fungal infections
CANDIDOSIS (CANDIDIASIS)
Candidosis is an opportunistic infection. The most common causative agent, Candida albicans , is part of the normal oral microflora and only causes disease when there is an imbalance in the oral environment or when the host’s defenses are compromised.
- Some 50% of the normal population harbor Candida albicans as a normal oral commensal (without disease) and are termed “Candida carrieres”.
- C. albicans resides particularly on the posterior dorsum of tongue.
- Candida carriage is more frequent in
- Women
- People:
- of blood group O and with non-secretion of blood antigens in saliva
- of high carbohydrate diets causing acidic saliva
- with xerostomia
- on broad spectrum antimicrobial use
- who wear dental appliances
- who smoke tobacco
- who are immunocompromised (HIV, malnutrition, diabetes)
- who are hospitalised
- Candidiasis (candidosis) is the state when candida species cause lesions (host defences are compromised).
- C. albicans is the only common cause of oral fungal or yeast infection.
- Symptomatic candidiasis presents as mainly:
- White lesions (thrush, candidal leukoplakia and chronic mucocutaneous candidiasis) in which hyphal forms are common.
- Red lesions (denture-related stomatitis, median rhomboid glossitis, erythematous candidiasis) in which yeasts forms predominate.
Factors PREDISPOSING to ORAL CANDIDIASIS
These factors disrupt the normal oral flora or suppress the immune system, particularly T-cell responses.
- Local factors influencing oral immunity or ecology include:
- Xerostomia
- Smoking
- Broad-spectrum antimicrobials
- Corticosteroids
- Dental appliances
- Irradiation involving the mouth or the salivary glands
- Systemic immune defects, such as those caused by:
- Extremes of age
- Malnutrition
- Cytotoxic chemotherapy
- Immune T-cell defects (HIV infection, lymphoma, leukemia, cancer and PMNL defects, diabetes and immunosuppressant drugs)
- Anemia Microscopic image of filamentous bacteria stained with acid-fast technique.
Thrush
- Acute pseudomembranous candidiasis
- Called Pseudomembranous because it is easily removed
- It is termed because the white flecks resemble the appearance of the breast of the of the bird of that name
- Happens in newborns, can infect the newborn as well as the mother
- Antifungal cream for breastfeeding and for mouth
ACUTE ATROPHIC CANDIDIASIS
- Acute atrophic candidiasis presents as a red patch of atrophic or erythematous raw and painful mucosa, with minimal evidence of the white pseudomembranous lesions observed in thrush.
- Antibiotic sore mouth, a common form of atrophiccandidiasis, should be suspected in a patient who develops symptoms of oral burning, bad taste, or sore throat during or after therapy with broad-spectrum antibiotics.
- Patients withchronic iron deficiency anemia may also develop atrophic candidiasis. Symptoms can include an oral burning sensation, a bad taste, or a sore throat.

Chronic hyperplastic candidiasis
- Candidal leukoplakia is considered a chronic form of oral candidiasis in which firm white leathery plaques are detected on the cheeks, lips, palate, and tongue. (persistent white lesion) characterized histologically by parakeratosis and chronic intrepithelial inflammation with fungal hyphae invading the superficial layers of the epithelium.
- Some have considered this as a precancerous lesion, although this is controversial with the latest literature
- The number of people affected is quite large and the amount of cancerous transformation isn’t significant
The surface of the plaque may be lobulated or fissured. A key diagnostic step is to see if the lesion resolves after antifungal treatment; if it does not, a biopsy is required to rule out dysplasia or malignancy.

- The number of people affected is quite large and the amount of cancerous transformation isn’t significant
The surface of the plaque may be lobulated or fissured. A key diagnostic step is to see if the lesion resolves after antifungal treatment; if it does not, a biopsy is required to rule out dysplasia or malignancy.
Angular Cheilitis
- Angular cheilitis is chronic inflammation affects both commissure of the lips
- Common
- Occurs mostly in adults
- It is predisposed by “3Ds”
- Denture-wearing, denture related stomatitis and disorders (dry mouth, tobacco smoking)
- Deficiency states (deficiency anemias, iron deficiency, hypovitaminosis (B), malabsorption states or eating disorders, zinc deficiency, immunity disorders)
- Disorders where the lip anatomical relationship are changed (reduced vertical dimension)
- A reduced vertical dimension, often from tooth loss or worn dentures, causes saliva to pool in the corners of the mouth, creating a moist environment for fungal growth. - A swab can be used to confirm the presence of Candida , and treatment typically involves the application of topical antifungal creams. There is no text in this image.
Denture-related Stomatitis
Aetiology and Pathogenesis
- Candida proliferates in the dental plaque, dental appliance surface and on the mucosa.
- Most common in patients who don’t remove their oral appliances at night
- An ill-fitting denture can cause mechanical irritation and create an environment conducive to fungal growth.
- Absence of symptoms
- Chronic erythema and edema of the mucosa that contacts the fitting surface of the denture
- Uncommon complications which include:
- Angular stomatitis
- Papillary hyperplasia in the palate
Histopathology
Diagnostic Methods
- Swab : A sterile cotton bud is used to collect a sample for laboratory culture.
- Cytology Smear : Cells are scraped from the lesion, placed on a glass slide, and stained with Periodic acid-Schiff (PAS) stain , which highlights the fungal hyphae in a magenta color.
Microscopic Features
- A key diagnostic feature is the presence of neutrophil microabscesses within the superficial layers of the epithelium.
- The epithelium may be atrophic (thinned), as seen in atrophic candidiasis, or hyperplastic (thickened) with parakeratosis and acanthosis, as seen in chronic hyperplastic candidosis.
- In all cases, Candida hyphae can be seen invading the superficial layers of the epithelium. Black arrows are epithelial cells infected by viruses