Oral Pathology module
Bone and Metabolic Disorders
Tori and Exostosis
Tori
- 2-10% of adults;
- Clinically: exophytic, hard, uninodular or multinodular bony masses covered by mucosa that may be ulcerated from trauma;
- torus palatinus and torus mandibularis on the midline of palate and lingual mandible (usually bilateral and symmetric), respectively;
- Can cause issues when fitting dentures, patients may even need to receive reconconstructive surgery to make the ridges appropriate for the denture
- often site of bisphosphonate-associated osteonecrosis
Exostoses
- 27% of adults;
- male predilection (5 : 1);
- Clinically: outgrowths of bone, nodular or sessile frequently on buccal aspects of mandible and maxilla or ascending arch of the palate and more than 90% having concurrent tori
Possible aetiology
- Chronic irritation
- Periosteal proliferation
- Bone formation
Differential diagnosis
- Biopsy is not necessary unless the lesion is radiographically progressive; histopathology is similar, and bone is often sclerotic.
- DD:
- Condensing osteitis is similar to idiopathic osteosclerosis but is found at or very close to the apices of teeth and is likely reactive to chronic occlusal trauma or low-grade inflammation or odontogenic infection.
- True osteomas are associated with (autosomal dominant condition associated with mutation in the APC gene and development of colonic polyps and carcinoma, desmoid tumors, supernumerary teeth, and skin cysts).
Osteomyelitis
Definition
- inflammatory condition of the bone, which begins as an infection of the medullary cavity, rapidly involves the haversian systems, and extends to involve the periosteum of the affected area
- Only 2 out of every 10,000 people get osteomyelitis.
Predisposing factors
- Diabetes (most cases of osteomyelitis stem from diabetes)
- Sickle cell disease
- HIV or AIDS
- Rheumatoid arthritis
- Intravenous drug use
- Alcoholism
- Long-term use of steroids
- Hemodialysis
- Poor blood supply
- Recent injury
Osteomyelitis of the Jaws
- The potential source of infection is
- Periapical infection
- Periodontal pocket’s
- Acute gingivitis
- Penetrating and contaminated injuries
- Tooth extraction
Signs and symptoms
- Fever, irritability, fatigue
- Nausea
- Tenderness, redness, and warmth in the area of the infection
- Swelling around the affected bone
- Lost range of motion
Classification
- Acute osteomyelitis is mainly in children (acute process occurs up to one month after the onset of symptoms)
- Chronic osteomyelitis (mainly adults)
- primary chronic osteomyelitis (PCO) is defined as chronic non-suppurative osteomyelitis; when PCO occurs in children and adolescents it is termed ‘Garré’s osteomyelitis’.
- secondary chronic osteomyelitis (SCO), which is chronic osteomyelitis with suppuration, abscess/fistula formation, and sequestration at some stage of the disease due to a defined, infectious aetiology.
Classification Systems Comparison
| Reference | Classification | Classification criteria |
|---|---|---|
| Hjorting-Hansen E Decortication in treatment of osteomyelitis of the mandible. Oral Surg Oral Med Oral Pathol 1970 May;29(5):641-55 | I. Acute/subacute osteomyelitis II. Secondary chronic osteomyelitis III. Primary chronic osteomyelitis | Classification based on clinical picture and radiology |
| Mercuri LG Acute Osteomyelitis of the Jaws Oral and Maxillofacial Surgery Clinics of North America, Vol 3, No 2, May 91, 355-65 Marx RE Chronic Osteomyelitis of the Jaws Oral and Maxillofacial Surgery Clinics of North America, Vol 3, No 2, May 91, 367-81 | I. Acute osteomyelitis 1. Associated with Hematogenous spread* 2. Associated with intrinsic bone pathology or peripheral vascular disease* 3. Associated with odontogenic and nonodontogenic local processes* II. Chronic osteomyelitis 1. Chronic recurrent multifocal osteomyelitis of children 2. Garre's osteomyelitis 3. Chronic suppurative osteomyelitis - Foreign body related - Systemic disease related - Related to persistent or resistant organisms 4. True chronic diffuse sclerosing osteomyelitis | Classification based on clinical picture and radiology, etiology, and pathophysiology Classification of acute osteomyelitis by Mercuri, classification of chronic osteomyelitis by Marx. The arbitrary time limit of one month is used to differ acute from chronic osteomyelitis * From Waldvogel and Medoff 1970 |
| Panders AK, Hadders HN Chronic sclerosing inflammations of the jaw. Osteomyelitis sicca (Garre), chronic sclerosing osteomyelitis with fine-meshed trabecular structure, and very dense sclerosing osteomyelitis. Oral Surg Oral Med Oral Pathol 1970 Sep;30(3):396-412 | I. Primarily chronic jaw inflammation 1. Osteomyelitis sicca (synonymous osteomyelitis of Garrè, chronic sclerosing nonsuppurative osteomyelitis of Garrè, periostitis ossificans) 2. Chronic sclerosing osteomyelitis with fine-meshed trabecular structure 3. Local and more extensive very dense sclerosing osteomyelitis II. Secondary chronic jaw inflammation III. Chronic specific jaw inflammations - Tuberculosis - Syphilis - Lepra - Actinomycosis | Classification based on clinical picture and radiology Classification of chronic osteomyelitis forms only |
Pathogenesis of Mandibular Osteomyelitis
Inflammation causes thrombosis of vessels in the marrow, ‘peri-osteal stripping’ by pus (or surgery) causes loss of peri-osteal blood supply, with consequent bone necrosis. This encourages continuance of infection as well as bone resorption.
Alveolar ostitis ( Dry socket)
- Localized inflammation of bone following either failure of blood clot to form in socket, or premature loss or disintegration of clot. Unpredictable complication of tooth extraction (~1-3%).
Etiology
- Failure of blood clot formation due to Poor blood supply as in:
- Paget’s disease.
- Osteopetrosis.
- Following radiotherapy.
- Excessive use of vasoconstrictor in local anesthesia.
- Premature loss of blood clot may be due to:
- Excessive mouth rinsing.
- Fibrinolysis by proteolytic bacteria.
Histopathology
- Histological section of socket wall reveal formation of necrotic bone containing empty lacunae
Osteonecrosis
- Osteoradionecrosis
- Osteochemonecrosis (corticosteroids and other cancer and antineoplastic drugs)
- MRONJ (medication-induced osteonecrosis)
- BRONJ (bisphosphonate-induced osteonecrosis)
- Phosphorous necrosis of the jaw (exposure to white phosphorous)
- The mandible specifically is most susceptible to osteonecrosis
Osteoradionecrosis and Radiosteomyelitis
- Radiotherapy in HNSCC
- Osteoradionecrosis was once considered an infection initiated by bacteria, which invaded the radiation-damaged bone
- The term “radiation-induced osteomyelitis” or radio-osteomyelitis was commonly used. Marx (1983)
- Radiation
- HNSCC
- Bone
- Hypoxia
- Hypocellular
- hypovascular
- Trauma
- Chronic non-healing wound
- Susceptible to superinfection
Biologic Action of Bisphosphonates
- Osteoclastic toxicity
- Apoptosis
- Inhibited release of bone induction proteins
- BMP, ILG1, ILG2
- Reduced bone turnover, resorption
- Reduced serum calcium*
- Hypermineralization*
- “sclerotic” changes in lamina dura of alveolar bone
- = goal of medicinal use Clinical image showing extensive necrosis of the lower gingiva and alveolar mucosa. Panoramic dental X-ray showing teeth and jaw structure. Microscopic image of bone tissue.
Position Paper: Medication-Related Osteonecrosis of the Jaw---2014 Update
Special Committee on Medication-Related Osteonecrosis of the Jaws:
Introduction
Research and Evidence
World Workshop on Oral Medicine VI: Controversies regarding dental management of medically complex patients: assessment of current recommendations.
- Dental recommendations for patients with certain medical conditions (osteoporosis, cardiovascular diseases, prosthetic joints, steroid use) often lack strong evidence.
- Expert opinion suggests minimal dental treatment modification for osteoporotic patients on bisphosphonates and general surgery guidelines are often applied to dentistry for CVDs.
Key Recommendations for Dental Management of Patients on Bisphosphonates for Osteoporosis
| Recommendation | Level of evidence* | Class of recommendation† |
|---|---|---|
| In all patients, clinicians should discuss: | ||
| - Importance of maintaining good oral hygiene¹⁹ | NA | NA |
| - Lifestyle changes, such as smoking cessation for those at high risk for MRONJ¹⁹ | NA | NA |
| - Very rare occurrence of MRONJ¹⁹ | NA | NA |
| Risk assessment and treatment planning - Potential risk factors for MRONJ: | ||
| Oral risk factors: | ||
| - Recent dentoalveolar trauma⁹¹⁻⁹³ | NA | NA |
| - Dental extraction⁹⁰,⁹¹ | NA | NA |
| - Dentoalveolar surgery⁹¹ | NA | NA |
| - Poor oral hygiene⁹¹ | NA | NA |
| - Oral infections⁹¹ | NA | NA |
| - Periodontal disease⁹¹ | NA | NA |
| Systemic risk factors: | ||
| - Greater frequency of administration⁹¹ | NA | NA |
| - Larger BP dose⁹¹ | NA | NA |
| - Longer treatment regimens⁹¹ | NA | NA |
| - Radiation therapy⁹¹ | NA | NA |
| - Infectious disease⁹¹ | NA | NA |
| - Concomitant therapy with corticosteroids⁹⁰,⁹² | NA | NA |
| - Compromised immune status or immunodeficiency⁹² | NA | NA |
| - Advanced age⁹² | NA | NA |
| - Chronic diseases⁹² | NA | NA |
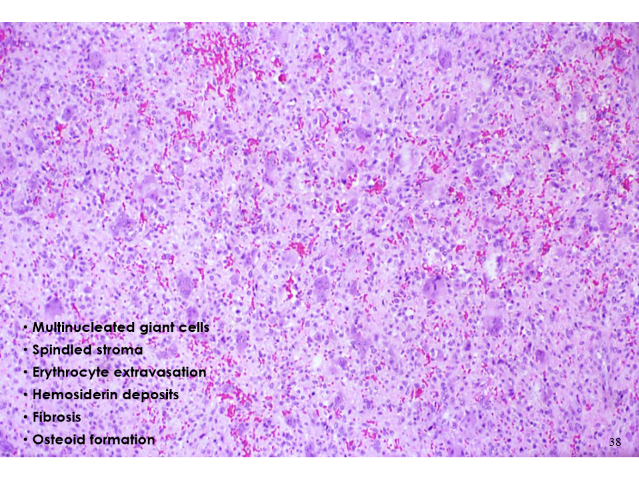
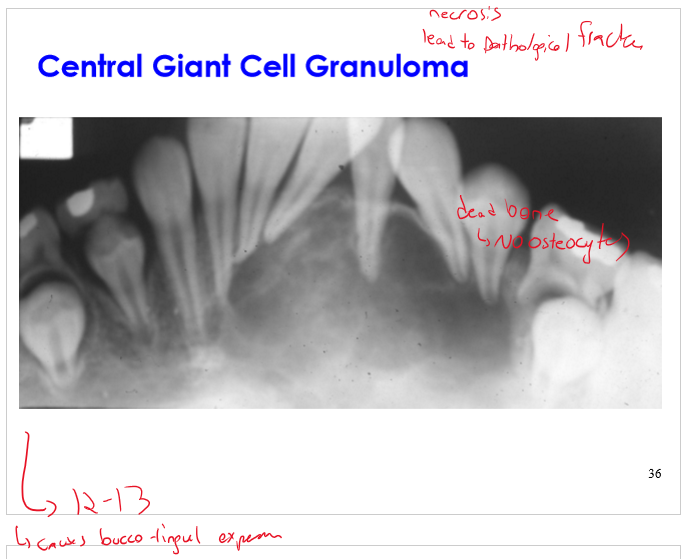
Central Giant Cell Granuloma
Histological Features
- Multinucleated giant cells
- Spindled stroma
- Erythrocyte extravasation
- Hemosiderin deposits
- Fibrosis
- Osteoid formation
Histological image showing densely packed cells with pleomorphic nuclei and areas of inflammatory infiltrate.
Clinical Features
- Etiology: non-neoplastic — reactive lesion
- Age: wide range (60% < 30 years of age)
- Gender: female > male
- Site: anterior mandible (70%)
- Symptoms: painless expansion
- Radiograph:
- unilocular to multilocular radiolucency
- 0.5 — 10.0 cm
Central Giant Cell Lesion
Differential Diagnosis:
- Central giant cell granuloma
- Brown tumor — hyperparathyroidism
- Aneurysmal bone cyst
- Cherubism
- Giant cell tumor
- Benign fibro-osseous lesion
Hyperparathyroidism
- Brown tumour (osteitis fibrosa cystica)
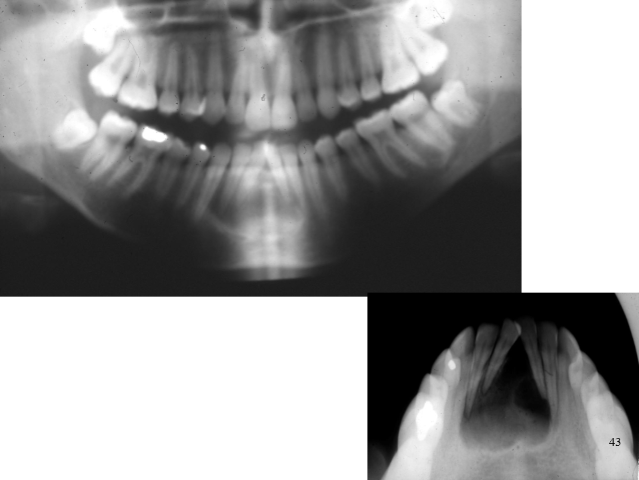
Case Report: Total Resolution of hyperparathyroidism-related jaw lesion by Vitamin D therapy
Can Vitamin D Therapy Contribute to the Conservative Resolution of Osteolytic Lesions of the Jaws? Clinically Relevant Summary --- Case Report
- Patient: 12-year-old girl with painless left mandibular swelling; radiograph showed radiolucent lesion in premolar/molar area.
- Differential diagnosis initially: odontogenic cyst or tumor, giant cell lesion.
- Workup finding: secondary hyperparathyroidism caused by severe vitamin D deficiency.
- Treatment:
- Single intramuscular vitamin D dose (300,000 IU)
- Oral vitamin D (10,000 IU weekly)
- Outcome:
- 6 weeks: normalization of vitamin D and parathyroid hormone (PTH) levels, marked clinical/radiologic improvement.
- 18 months: complete radiographic resolution of lesion, stable normal labs.
- Key point: Jaw osteolytic lesions can result from metabolic bone disease due to vitamin D deficiency.
- Clinical recommendation: Rule out systemic causes (esp. vitamin D deficiency with secondary hyperparathyroidism) before surgical management to avoid unnecessary operations. A B C D E
Benign cemento-osseous lesions
- Fibrous dysplasia
- Fibro-osseous lesions replace bone structure with tissue, this tissue will then calcify, the calcification can follow different patterns (such as those of bone or cementum), this leads to the various different kinds of fibrous dysplasias
- Cemento-osseous dysplasias
- Subtypes: periapical cemental, focal cemento-osseous, florid cemento-osseous
- Cemento-ossifying fibroma
- Subtypes: conventional, juvenile active
Fibrous Dysplasia
- Benign disorder of bone
- Non-neoplastic tumor-like lesion
- Developmental defect in bone formation
- Fibrous proliferation
- Disorderly malformed woven bone
- Enlarged deformed bones
- Structurally weak
- Sites: ribs, femur, tibia, pelvis, craniofacial
- Age: onset in childhood - adolescence
- Single or multiple bony lesions
- Slow growing
- Painless
- Often quiesces at puberty
- Genetics: GNAS I gene chromosome 20q13.1-2
- CAN CAUSE DEFORMITIES TO THE FAC E
Types of Fibrous Dysplasia
- Monostotic - 70%
- craniofacial — (25%)
- Polyostotic - 25%
- craniofacial — (50%)
- McCune-Albright Syndrome - 3%
- endocrine abnormalities
Oral & Maxillofacial Manifestations
- Painless swelling
- Facial asymmetry
- Malocclusion — displaced teeth
- Headache
- Hearing loss
- Clinical labs: elevated alkaline phosphatase
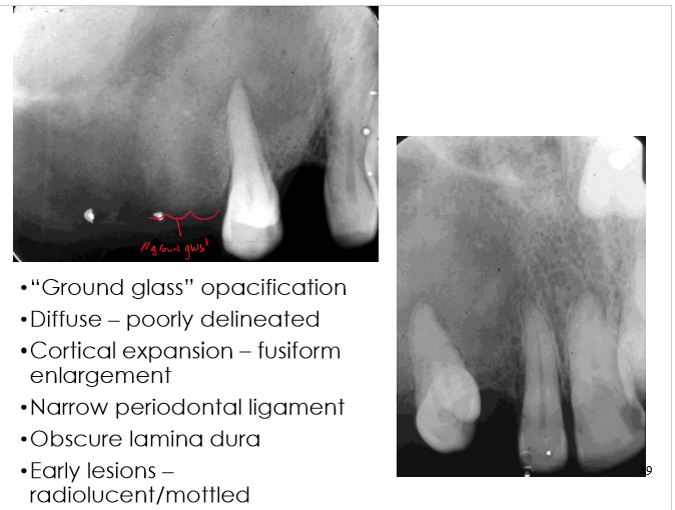
Radiographic Features
- “Ground glass” opacification
- Diffuse — poorly delineated
- Cortical expansion — fusiform enlargement
- Narrow periodontal ligament
- Obscure lamina dura
- Early lesions — radiolucent/mottled
Periapical Cemento-Osseous Dysplasia
- Benign non-neoplastic dysplastic process
- Incidence: relatively common
- Age: middle age (30 — 50 years)
- Gender: female > male (14:1)
- Race: black
- Site: mandibular anterior — periapical area
- Asymptomatic, vital teeth, non-expansile
- This is important as all the teeth are all vital, so even though it looks like a periapical lesion, we should be thinking about cemento-osseous dysplasia Dental radiograph showing the roots of multiple anterior teeth.
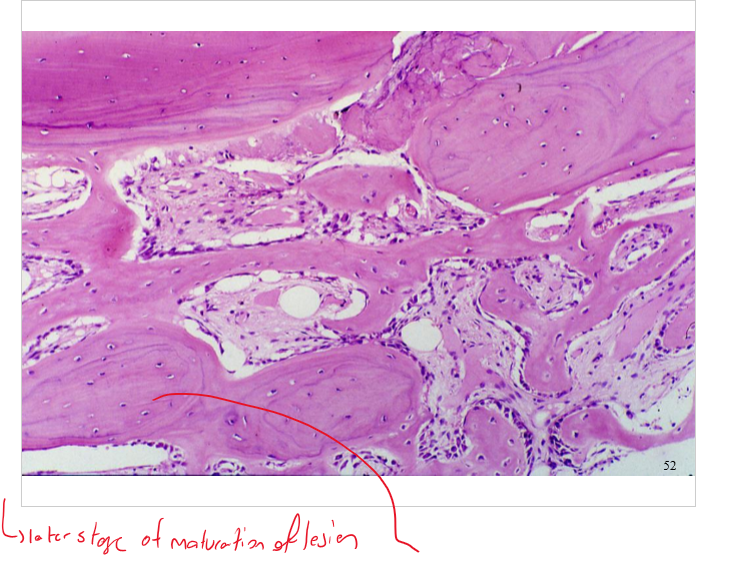
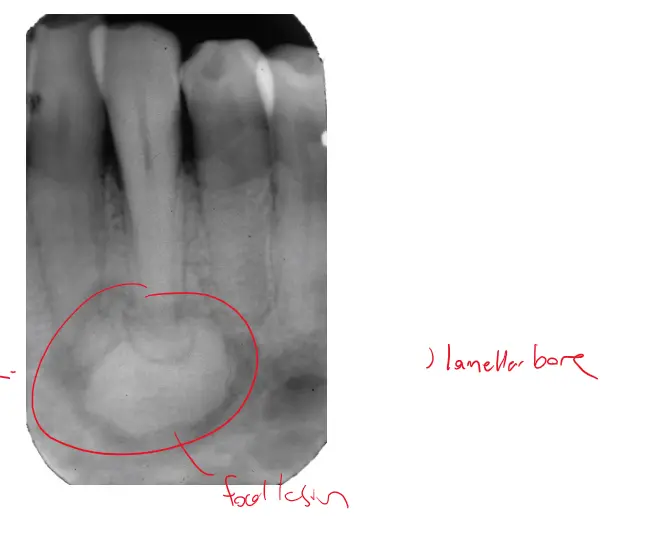
Focal Cemento-Osseous Dysplasia
- Etiology: non-neoplastic — disordered growth of cementum and bone
- Incidence: most common benign fibro-osseous lesion
- Age: 4-5th decade
- Gender: female (80%)
- Race: Caucasian
- Site: posterior mandible
- Asymptomatic
- Solitary
- Edentulous areas
- Size: < 1.5 cm
- Radiographic: mixed radiolucent — opaque, well-defined or irregular borders
- Usually focal affects a specific quadrant only
Radiographic and histologic images labeled “FCOD” (Focal Cemento-Osseous Dysplasia).
Florid Cemento-Osseous Dysplasia
Clinical Features
- Benign non-neoplastic dysplastic process
- Incidence: relatively rare
- Age: middle-aged adults
- Gender: female > male
- Race: black (90%)
- Site: diffuse involvement of jaws
- Asymptomatic, expansion, secondary infection
- These patients are considered high risk for osteomyelitis it is high risk
Radiographic Features
- Irregular lobular dense radiopacities
- Mixed radiolucent and radiopaque areas
- Diffuse involvement of maxilla and mandible
- Bilateral
- Symmetrical
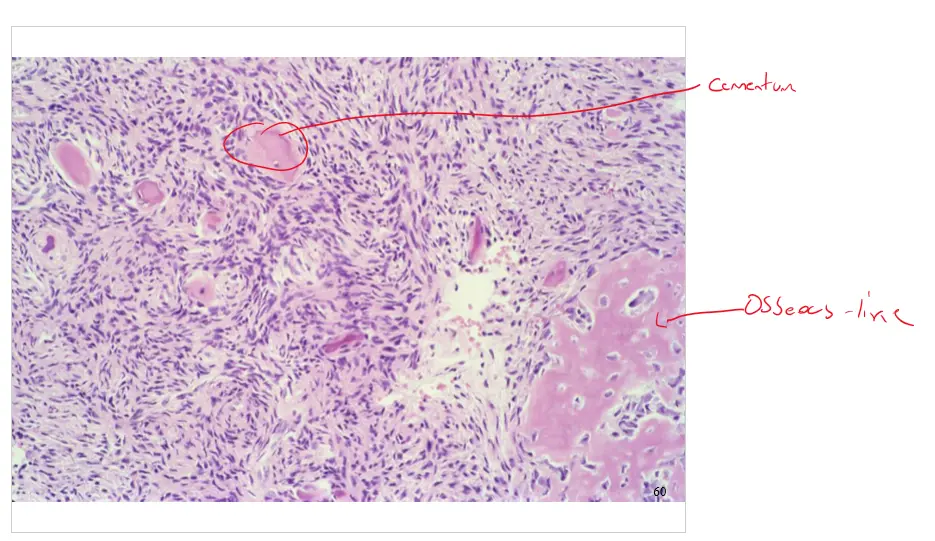
Histological Features
- Fibroblastic proliferation
- Dense sclerotic calcific masses
- Cementum matrix
- Woven bone
- Inflammatory infiltrate
Osteoma
- Benign bone forming tumor
- Reactive — developmental (non-neoplastic)
- Site: craniofacial bones: skull, paranasal sinuses
- Solitary exophytic mass of dense bone arising from periosteal or endosteal surface
- Asymptomatic
- Non-aggressive, no malignant transformation Oral soft tissue lesion on the upper gingiva near the molars.
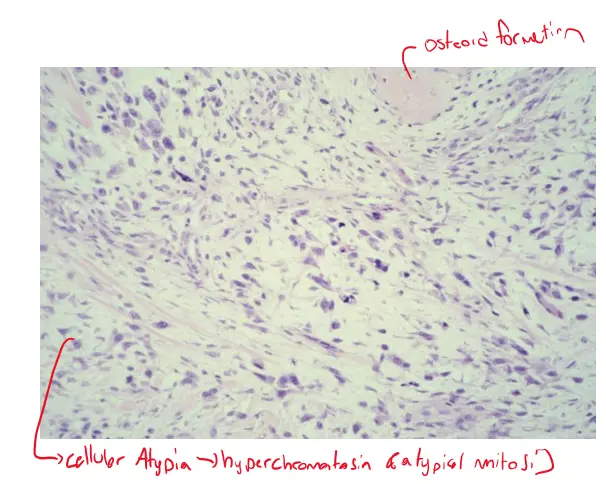
Osteosarcoma of Head & Neck
- Incidence: rare in the jaws
- 6-8% occur in the gnathic skeleton
- Age: 3-4th decade (mean age 33 years)
- Gender: male > female
- Site: mandible = maxilla, paranasal sinuses, skull
- Symptoms: painful swelling, paresthesia, loose teeth
- Every patient that complains of paresthesia should be treated as a serious case , it is a very red flag
Facial swelling (likely parotid or mandibular region)
- Every patient that complains of paresthesia should be treated as a serious case , it is a very red flag
Facial swelling (likely parotid or mandibular region)
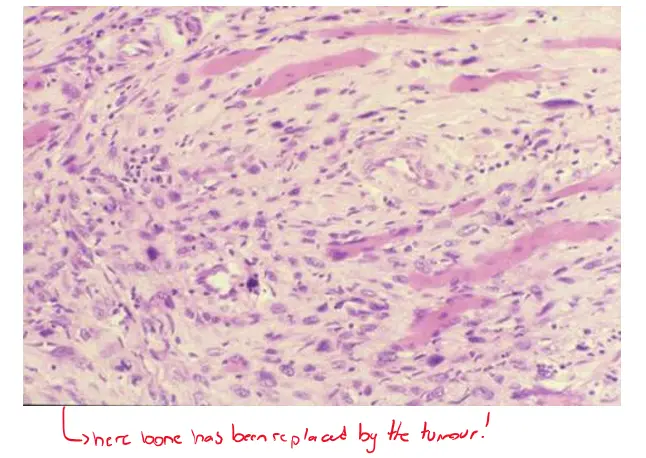
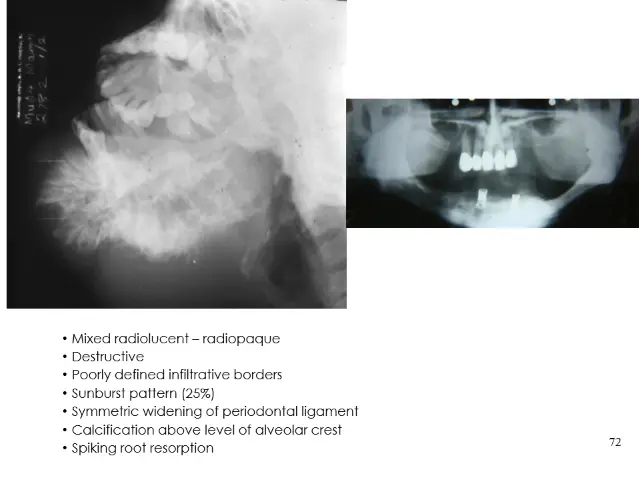
Radiographic Features
- Mixed radiolucent — radiopaque
- Destructive
- Poorly defined infiltrative borders
- Sunburst pattern (25%)
- Symmetric widening of periodontal ligament
- Calcification above level of alveolar crest
- Spiking root resorption Histological image with spindle-shaped cells and fibrous stroma
Metastatic Tumours to Bone
- Most common form of cancer involving bone
- Carcinomas
- Breast, prostate, lung, kidney, thyroid
- Site: vertebral column, pelvis, ribs, skull Central Giant Cell Granuloma
- Poor prognosis
Metastatic Tumours to the Jaws
- Radiographic features:
- osteolytic: ill-defined destructive radiolucency
- osteoblastic: radiopaque or mixed lesion
- May simulate periapical or periodontal disease
- Histology: infiltrating nests and cords of pleomorphic epithelial cells with fibrous stroma
- Prognosis: poor, widely disseminated disease
- Survival: less than one year Histological image of glandular tissue with abnormal architecture.