Superseded as the canonical RPD overview
The full RPD synthesis (covering classification, components, biomechanics, surveying, and the clinical workflow) now lives at Removable Partial Dentures Overview. The Maxillary, Mandibular, and General Maxillary Design Principles sections below — along with the Recommended Major Connector by Kennedy Class table — have been merged into that note verbatim.
This file is retained as a focused deep-dive into mandibular major connector indications and drawing tips. Use the canonical overview as your study landing page; come here only when you need the original footnoted detail on a specific mandibular connector.
Mandibular Connectors 12 34
-
The mandibular connectors are as follows
-
- Lingual bar
- Lingual bar with cingulum bar (continuous bar)
-
- Labial bar Mental Dentals Section on Mandibular Major Connectors - which most of this is based on!
-
-
In general (needs fact checking) it seems as though mandibular major connector selection is guided by anatomic considerations more so than Kennedy classes (i.e. we need a reason to not use a lingual bar, otherwise just keep it simple )
{kind=link}
{kind=link}
{kind=link}
{kind=link}
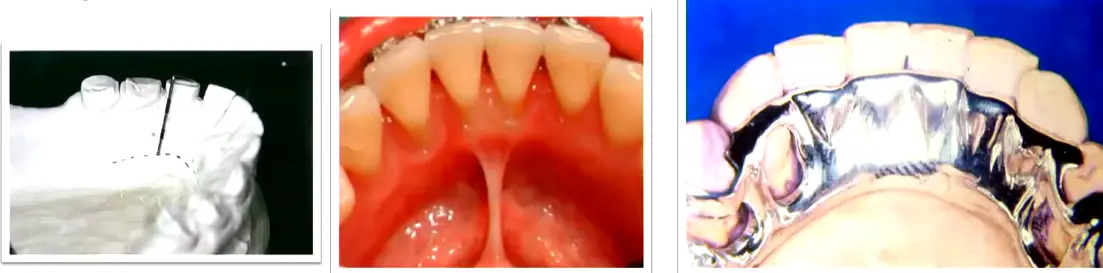
Lingual Bar
**Indications for Lingual Bar :
- When depth of the lingual vestibule is >= 7mm
- ==Simplest and most common mandibular major connector
Vestibular space is very important in this regard
“At least two clinically acceptable methods may be used to determine the relative height of the floor of the mouth and locate the inferior border of a lingual mandibular major connector.” (Carr and Brown, 2015, p. 33) (pdf)
- The first method is to measure the height of the floor of the mouth in relation to the lingual gingival margins of adjacent teeth with a periodontal probe
7 mm is a good estimation by mental dental, but McKrakens insists that its just enough so that the bar does not impinge on the tissue in the floor of the mouth .
- the lectures on the other hand recommend 8mm of space 4 for a bar height of 5 mm and a minimal clearance of 3 mm from the gingival margin
Drawing tips 5
- Maintain 0.3–0.5 mm clearance from the lingual tissue
- Place the bar 3–5 mm below the gingival margins
- If a deep soft-tissue undercut is present, the lingual bar may create a food trap or speech impediment — a linguoplate is the better choice in that situation 5
Lingual Plate
Indications 6
- when the lingual frenum is high or the space available for a lingual bar is limited
- In Class I Situations in which the residual ridges have undergone excessive vertical resorption
- For stabilizing periodontally weakened teeth
- When the future replacement of one or more incisor teeth will be facilitated by the addition of retention loops to an existing linguoplate
“Generally, the apron is used to avoid gingival irritation or entrapment of food debris or to cover generously relieved areas that would be irritating to the tongue” (Carr and Brown, 2015, p. 35) (pdf)
Other Mandibular Major connectors
generally very rare, used in cases where the teeth are very tilted or there are extensive hard/ soft tissue undercuts
7
Sublingual Bar
- Shallow floor of mouth
- Lingual undercuts
- Low frenulum attachment
- Lingual tori
- Essentially a lingual bar placed more posteriorly and inferiorly
- Lies over and parallel to the anterior floor of mouth
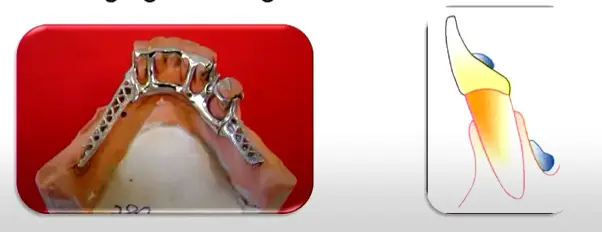
Double Lingual Bar (Kennedy Bar)
- Standard lingual bar + a secondary bar above the cingula, where additional indirect retention or splinting of periodontally involved teeth is desired
- Across the anterior teeth in Class II/III cases when additional stability is needed but leaving the gingival margins open is desirable 89
- Distributes oblique loads across multiple teeth rather than concentrating them on a single rest
- Key advantage vs linguoplate: provides stability while leaving the gingival margins open for self-cleansing 9
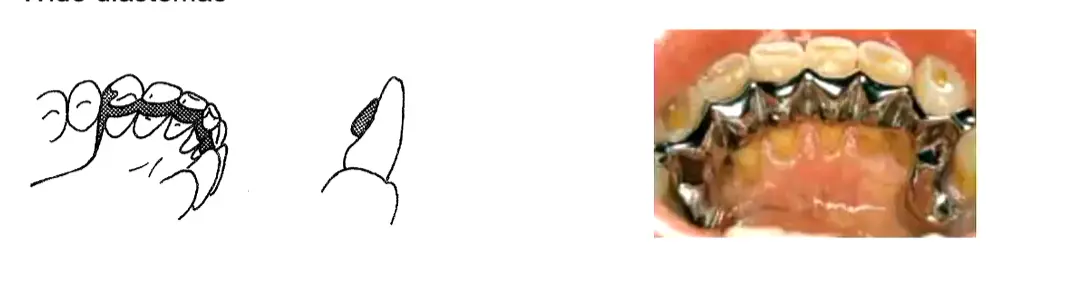
- Contraindicated where diastemas exist — exposed metal would be visible through the gaps
- Tendency to trap food debris; multiple borders may irritate the tongue
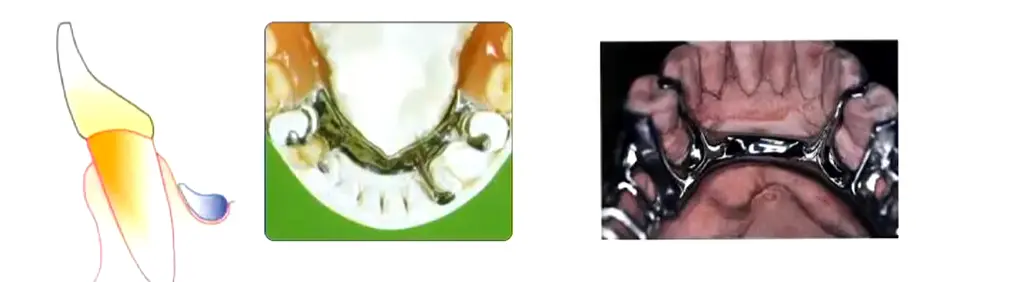
Cingulum Bar (Continuous Bar)
Indications 4
- Only when clinical crowns are long enough and no alternative connector is feasible
Drawing tips 4
- Contraindicated on retroclined anterior teeth or where wide diastemas are present
Labial Bar (Swing-Lock)
Indications 3
- Missing canine
- Unfavourable lingual soft-tissue contour
- Questionable periodontal prognosis
Drawing tips 3
- Swing-lock variant incorporates a hinge at one end and a locking mechanism at the other
Maxillary Major Connectors
Single Palatal Strap
{kind=link}
- Kennedy Class III without anterior modification
- ≥ 8 mm wide for rigidity, kept thin for tongue comfort
- Borders follow the valleys of the rugae rather than crossing over them
- Both anterior and posterior borders should cross the midline at right angles for optimal rigidity
Anterior-Posterior Palatal Strap
{kind=link}
- Kennedy Class II, Class III with anterior modification, and Class IV
- Preferred “closed oval” skeletal design for Class I long distal-extension spans — excellent rigidity 10
- Each strap ≥ 8 mm wide, flat profile
- Posterior strap placed anterior to the hard/soft palate junction — avoids the vibrating line and the gagging/instability that results from crossing it
- The overall width of the connector should correspond roughly to the amount of posterior occlusion being replaced 8
- Minimise coverage of the anterior rugae to preserve sibilants (/s/, /z/) and alveolar sounds (/t/, /d/)
- Contraindicated where an inoperable torus extends onto the soft palate
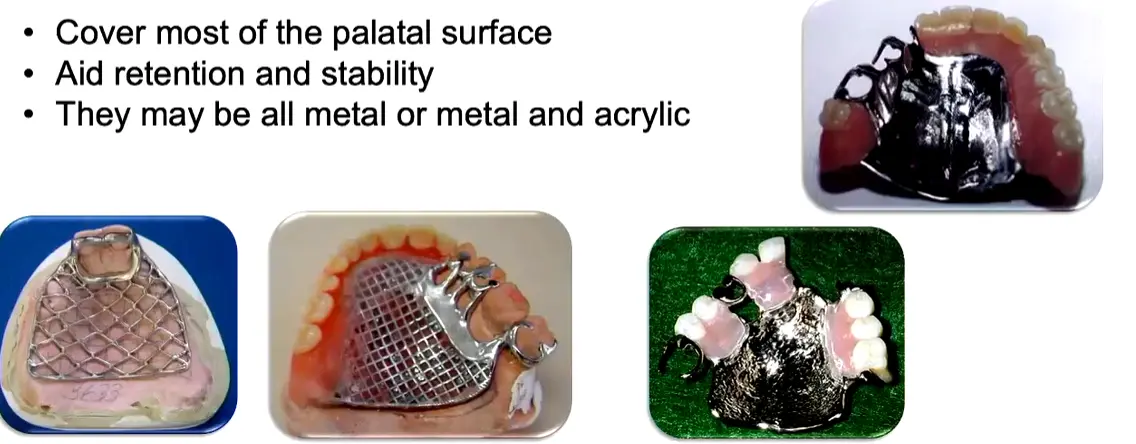
Palatal Plate (Complete Palatal Coverage)
{kind=link}
- Few remaining teeth (e.g. only anterior teeth present)
- Remaining teeth with a guarded prognosis
- Long, flat or flabby residual ridges; shallow vaults; small mouths
- Most common choice for Kennedy Class I 3
- Long-span Class IV (“pseudo-Class V” — 6–8 anterior teeth missing), where a horseshoe is often insufficient and palate depth or a prominent mid-palatine raphe rules out a closed-oval strap 11
- Most rigid maxillary major connector — provides substantial retention/stability via intimate tissue contact
- All-metal vs metal + acrylic: metal conducts temperature, aiding patient adaptation and taste; only mesh/acrylic variants permit future relining
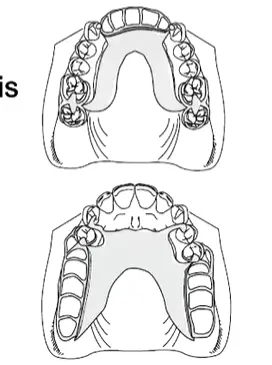
Horseshoe
{kind=link}
- Inoperable large palatal torus (patient declines surgical removal)
- Significant gag reflex
- Some Class IV presentations
- Poorest maxillary connector for rigidity — use sparingly
- Requires bulk in the rugae zone where tongue space is most valued
- Often insufficient for long-span Class IV — switch to a closed-oval A-P strap or a full palatal plate depending on palate depth and mid-palatine raphe prominence 11
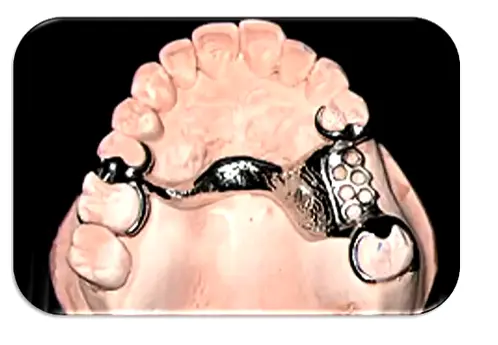
Single Palatal Bar
{kind=link}
- Kennedy Class III with a small edentulous span only
- Contraindicated in Class I and Class II (insufficient vertical support, poor rigidity)
- < 8 mm wide, narrow half-oval cross-section
- Do not place anterior to the 2nd premolar — profile is bulky
- Ideal placement is in the median region, behind the rugae
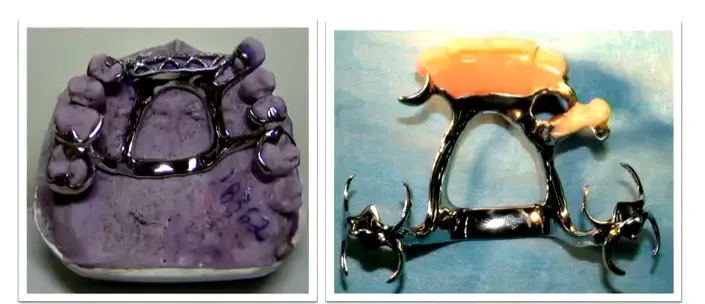
Anterior-Posterior Palatal Bars (Double Bar)
{kind=link}
- Absence of many teeth (anterior and posterior)
- Presence of a palatal torus
- Two flat longitudinal elements per side; the anterior portion is typically less bulky
- High rigidity with minimal soft-tissue coverage
- Multiple borders can be uncomfortable for the tongue
Maxillary General Design Principles
- All major connectors should cross the midline at right angles for maximum rigidity 3412
- Borders kept ≥ 6 mm from the gingival margins in the maxilla, ≥ 3–4 mm in the mandible 413; the Denture Adventure workflow uses a practical 3–5 mm rule around gingival margins and around the incisive papilla 912
- Avoid crossing major rugae with the connector border where possible 12
- Connector width scales with load: the overall width of a maxillary connector should roughly correspond to the amount of posterior occlusion being replaced 812
- Relief is required over the median palatal raphe — the midline suture is prominent and rigid, and settling there causes instability 4
- Beading (maxillary exclusive): a 0.5 × 1 mm rounded groove scribed on the master cast along the connector borders, fading out 6 mm from the gingival margin. Prevents food collection and produces a mechanical tissue seal. Narrow bars do not require beading; the clinician must explicitly specify beading to the laboratory. On duplication, the bead line is scored anteriorly and posteriorly but not across the median palatal suture or incisive papilla 3412
- Posterior limit of the connector must lie anterior to the vibrating line 13
- Relief by Kennedy class: Class III = none or minimal (tooth-supported); Class I, II, IV = moderate (~1.5 mm) 13
- Support correlation: the poorer the periodontal support of the remaining teeth, the greater the palatal coverage required 4
- Maintain smooth natural palatal contours — decorative rugae-simulation patterns irritate the tongue 4
- Long-span anterior modifications may require additional connector thickness or “strengtheners” to prevent midline flexion during function 9
Summary Table — Recommended Major Connector by Kennedy Class
| Kennedy Class | Maxillary | Mandibular |
|---|---|---|
| Class I | A-P Palatal Strap (“closed oval” — excellent rigidity) is the academic baseline; Palatal Plate when maximum mucosal support is needed or remaining teeth have a poor prognosis 310 | Lingual Bar (standard baseline); Linguoplate or Kennedy Bar when additional indirect retention or splinting of periodontally involved teeth is needed 10 |
| Class II | Palatal Strap, A-P Palatal Strap, or Palatal Plate — width scales with the amount of posterior occlusion being replaced 8 | Lingual Bar (first choice); Linguoplate (apron) if < 7–8 mm from floor of mouth to gingival margin; Kennedy Bar across the anteriors if extra stability is needed 8 |
| Class III | Palatal Strap (the vertical-support workhorse); Single Palatal Bar for a small edentulous span; A-P Palatal Strap when an anterior modification is present 249 | Lingual Bar (standard); Linguoplate/aproning where teeth have a poor prognosis or indirect retention is needed; Kennedy Bar for stability while leaving gingival margins open for self-cleansing 9 |
| Class IV | A-P Palatal Strap (closed oval) for standard spans; ==Horseshoe often insufficient for long spans== — escalate to closed-oval A-P strap or Palatal Plate depending on palate depth and mid-palatine raphe prominence 2411 | Lingual Bar with attention to lingually-inclined posteriors and ridge atrophy; Linguoplate (or interrupted lingual bar with cingulum plating at canines) where vertical resorption is significant 11 |
Footnotes
-
L5 Major and Minor Connectors ↩ ↩2 ↩3 ↩4 ↩5 ↩6 ↩7 ↩8 ↩9 ↩10 ↩11 ↩12 ↩13 ↩14 ↩15 ↩16
-
Prosthodontics - 11 - Major & Minor Connectors ↩ ↩2 ↩3 ↩4 ↩5 ↩6 ↩7 ↩8 ↩9 ↩10 ↩11
-
General Principles for Mandibular Design ↩ ↩2 ↩3 ↩4 ↩5 ↩6 ↩7 ↩8 ↩9 ↩10 ↩11 ↩12 ↩13 ↩14 ↩15 ↩16 ↩17 ↩18 ↩19 ↩20 ↩21 ↩22 ↩23 ↩24 ↩25 ↩26
-
ROLE OF MAJOR CONNECTORS IN CONTROL OF PROSTHESIS MOVEMENT > Mandibular Major Connectors > Lingual Bar ↩
-
ROLE OF MAJOR CONNECTORS IN CONTROL OF PROSTHESIS MOVEMENT > Mandibular Major Connectors > Design of Mandibular Major Connectors ↩
-
Cast Partial Denture Design Kennedy Class II ↩ ↩2 ↩3 ↩4 ↩5 ↩6 ↩7 ↩8
-
Cast Partial Denture Design Kennedy Class III ↩ ↩2 ↩3 ↩4 ↩5 ↩6 ↩7 ↩8
-
Cast Partial Denture Design Kennedy Class IV ↩ ↩2 ↩3 ↩4 ↩5 ↩6